


The plan for WHO supremacy over human health
By Paraschiva Florescu, ANH Intl mission facilitator, and Rob Verkerk PhD, founder, executive and scientific director, ANH-Intl | May 11, 2023
Who’s WHO?
Much has changed since the World Health Organization (WHO) was established in the wake of World War II. Like a newborn, the WHO was initially naïve and came in with noble intentions. It evolved its view of health, moving from one that was just the absence of disease, towards a more holistic concept, being a “state of complete physical, mental and social well-being”. At the heart of its Constitution it positioned “enjoyment of the highest attainable standard of health” as a fundamental right for every human being.
After two traumatic world wars, people recognised that a common patchwork of sovereign nations with shared ideals and priorities would be the best way of raising health standards around the world, while recognising that empowering individuals to take control of their own health would be a powerful step towards this goal. The Alma-Ata Declaration of 1978 makes a refreshing read. In particular: Principle IV, that reinforces the importance of the individual, as well as the collective, in planning and implementing their health care; and Principle VI, with a nod to Nuremberg and the Doctors’ Trial, requiring that primary health care must be based on “practical, scientifically sound and socially acceptable methods and technology”.
With the very recent, coercive manner by which C19 genetic vaccines were rolled out experimentally on the masses — many of these often desperate to regain livelihoods and be released from lockdowns — it’s clear that the WHO Constitutional principles and those from Alma-Ata, were disregarded (see here, or here).
Like a child transforming from innocent to nasty teenager, the WHO appears to have used the covid-19 crisis as a catalyst for an about-turn on its more altruistic and democratic approach.
In the case of a child, most cases can be put down to the negative influences coming from the immediate environment of that child – such as the parents and the local community. With an organisation, it’s not that different because it’s down to who controls it; and the control of organisations is heavily dependent on who’s funding them.
One of the biggest changes the WHO has seen in its 75 year history is a shift from funding by sovereign nations to funding from private parties. As of now, the bulk of the WHO’s funding comes from the Bill and Melinda Gates Foundation and two closely aligned vaccine-based non-profits funded by vaccine and pharma companies, the vaccine alliance GAVI and the global Coalition for Epidemic Preparedness Innovations or CEPI.
There’s no hiding – even on these organisation’s own websites – the incestuous interconnection between various governments and organisations including the Bill & Melinda Gates Foundation and the World Economic Forum (WEF). It’s no coincidence that the Gates Foundation is the second largest funder of the WHO, which is also helping to fund the WEF.
IHR amendments and the Pandemic Treaty: brief breakdown
Despite the seemingly positive intentions behind the WHO’s agenda, there are sinister forces at play threatening to take away national sovereignty, to remove free speech and to move towards an ever more centralised, globalised, authoritarian, undemocratic, and top-down system of control over humans and their health.
The mechanisms being used for this deeply disturbing shift towards, globalised ‘one health’ are two-fold. One relates to changes proposed to the existing International Health Regulations of 2005 (IHR) via amendments that are currently being negotiated. This is, in effect, the only internationally applicable regulatory system in force that aims to regulate coordinated responses to health threats. The second mechanism involves the introduction of a new ‘treaty’, namely the ‘WHO convention, agreement or other international instrument on pandemic prevention, preparedness and response’ (WHO CA+). With a name like that, it’s short form, the ‘Pandemic Treaty’, has been widely adopted for ease of reference.
Although two separate documents, the amendments and the Pandemic Treaty work in tandem. One, the former, states the ‘what’, while the latter, the ‘how’. The amendments dramatically extend powers to the WHO, redefine important concepts and broaden the context, while the Pandemic Treaty is concerned with the financing and governance required to support these amendments.
The International Health Regulations’ amendments
Among deeply disturbing changes to the IHR are:
- Article 12 gives the Director-General of the WHO, presently Dr Tedros Adhanom Ghebreyesus, full power in declaring a Public Health Emergency of International Concern (PHEIC), but also a PHERC, a public health emergency of “Regional Concern”. Most disconcerting is the addition of the word “potential” public health emergency, meaning there is no need for an actual health emergency. Anything could be justified as a ‘potential’ PHERC or PHEIC, why not even a ‘climate emergency’, for example?
- Currently the recommendations are non-binding as reflected in Articles 1 and 15, but the changes will remove their “non-binding” nature, making these recommendations binding and removing any flexibility, leading to potential conflicts of interest. Once binding, the WHO will have supremacy over any nation state. Sovereignty during a pandemic, real or manufactured, will have been eliminated. Nation states devolve to mere WHO “member states”.
- Introduction of a new Article 13A underlines that states must recognise the WHO as the “guidance and coordinating authority” and “undertake to follow WHO’s recommendations”. This Article also encourages the development of rapid approval guidelines for health products (including vaccines) and it is no surprise that we are already seeing legislative changes in the UK that seek to streamline clinical trials in order to make, say, vaccine approval, quicker and easier, such as here.
- The amendments also delete the words “full respect for the dignity, human rights and fundamental freedoms of persons” from Article 3 and replace them with principles of “equity, inclusivity, coherence and in accordance with […] differentiated responsibility of the State Parties”. In a matter of a few words, some of the important, enduring and universal principles of human rights, namely respect for dignity and the fundamental freedoms of the individual, are cast aside, being replaced with vague, undefined terms like ‘inclusivity’ and ‘coherence’. Reference to economic and social development also implies that differential emphasis will be applied to different populations.
- Article 15 originally was about temporary recommendations being issued if a PHEIC is declared. The amendment to this article now covers not just a PHEIC, but also any event that has “a potential to become a PHEIC”. Temporary recommendations can include “medical countermeasures” and as outlined above, these will become binding on WHO “member states”. This could be just the ticket for imposing mandatory vaccination programmes, for example.
- Annex 1 includes a new requirement of “member states” to communicate any risks and counter “misinformation and disinformation”, the same point also included in another clause within Annex 1 (7) that requires the WHO to strengthen its capacity to “counter misinformation and disinformation”. The WHO will become the ultimate, unaccountable and unelected arbiter of the science. It has already developed an ‘infodemic department’. This will aim to manage current and upcoming “infodemics”, defined as “too much information including false or misleading information in digital and physical environments during a disease outbreak”. The WHO, like many global agencies and media portals, is on a mission to tackle disinformation by silencing discourse, dissenting scientists and everything that causes “confusion and risk-taking behaviours”. This would presumably include exercising one’s right of refusal to an experimental vaccine on the basis that protocols that enhance natural immunity are used instead. This directly infringes upon our right to freedom of expression and receiving/imparting information under Article 19 of the International Covenant on Civil and Political Rights (ICCPR), Article 10 of the European Convention on Human Rights (ECHR), and Article 15 of the International Covenant on Economic, Social and Cultural Rights (ICESCR).
- Article 13 (5) states that once an emergency or a potential emergency is declared, WHO “member states” will have to hand over funds and commodities to the WHO. Moreover, any intellectual property will need to be granted to the WHO which in turn will have ownership of property and control of manufacturing of any commodities relevant to the emergency. The wording has been changed from ‘should’ to ‘shall’ – making it no longer a choice, but a requirement. This threatens the right to privacy under Article 17 of the ICCPR and Article 8 of the ECHR.
More simply put, the amendments to the IHR would give Dr Tedros Adhanom Ghebreyesus, the current Director-General, supreme power over decisions within the IHR that would affect all 190+ WHO “member states”, regardless of any dissenting opinions or disagreements among members. This decision to offer a single individual such powers needs to be very carefully considered in the light of the lack of the WHO’s transparency and accountability.
What about the individual in question? Let’s think of current WHO DG, Dr Ghebreyesus. He has an alleged track record for genocide against various tribes in the Tigray region of his home country of Ethiopia, a matter that was brought to the International Criminal Court by US economist and past-advisor to the Ethiopian government, David Steinman, in 2020.
For those who might have felt that the WHO’s declaration of the end of the C19 public health emergency earlier this month was the beginning of a transition back to pre-pandemic norms, it’s time to think again. Now is the time that the WHO and the globalists are setting out their stall for the next phase of their agenda.
The Pandemic Treaty
As we indicated above, the IHR amendments need to be interpreted alongside the ‘Pandemic Treaty’, which will, interestingly enough, not only be concerned with pandemics. It introduces globally the ‘One Health’ that was already being used by the US Centers for Disease Control and Prevention (CDC) (see Figure 1). The concept recognises the interdependence of human and animal health, and the connection with the environment. It speaks less (in fact not at all) to lab leaks and gain-of-function research that currently provides the most plausible explanation of how C19 came to be.
Through this One Health agenda, the WHO will have power to make decisions in matters relating to the environment (including greenhouse gas emissions, pollution, deforestation), animal health (e.g. livestock) and human health (including vaccinations, social determinants and population movement).There’s not a lot concerning health that the WHO wouldn’t have sway in. With these extended powers, the WHO could readily declare a climate or environmental emergency and enforce lockdowns. You may have wondered why governments have been trialling emergency alerts (see example here) of late. Are you prepared for another lockdown somewhere near you soon? (Side note: We’re definitely not planning for it, but we continue to look for ways to ensure our phones don’t receive such alerts!)

Figure 1. One Health Approach. Source: IS Global
The One Health approach is aligned with WHO’s linear and reductionist thinking that seeks to distill all potential solutions to one view of the underlying science, one view on the necessary medicines, and only one truth. This monolithic approach spells grave dangers for humanity given that it is bottom-up, decentralised, regionally-specific approaches to complex health problems that have always been shown to work. Top-down, ‘one size fits all’ approaches, especially ones twisted by conflicted interests, are doomed to failure. Only those who fail to look at the wider scientific picture are prepared to convince themselves that the WHO’s first global attempt at managing a pandemic, involving masks, lockdowns and genetic vaccines, was a success.
At its core, the WHO’s extended powers will lead to even more censorship and will dismantle the notion of consensus science built on a transparent, scientific method and silencing dissenting voices.
Some other important clauses to note within the Pandemic Treaty include:
- Article 4(17), which places the WHO in a ‘central role’ as the ‘directing and coordinating authority with supremacy over WHO “member states”
- Article 6 establishes a supply chain and logistics network
- Article 7 concerns the transfer of technology and pandemic-related products (including vaccines, therapeutics etc) and ‘time-bound waivers of intellectual property rights’. Given almost no separation between vaccine interests that fund the WHO and the WHO itself, this might give the impression of collective responsibility and lack of self-interest – but it’s more like passing the parcel among very close friends
- Article 8 brazenly casts aside the long-held view of the value of years of regulatory oversight in the approval of new technology and vaccines. It demands that countries accelerate the process of approval. This could infringe upon our right to health under Article 12 ICESCR as well as right to safe and effective medical products. This is already implemented by the CEPI campaign that seeks to accelerate vaccine approval to 100 days, instead of the prior vaccine approval process of 5-10 years. This move that has been catalysed by the arrival of mRNA technology could present serious and unknown consequences to the health and safety of the population.
- Article 12 seeks to build a ‘workforce’
- Article 15 reminds us again of the WHO’s central role as the global ‘directing and coordinating authority’
- Article 17 gives us a clearer understanding of the implications the treaty on our freedom. It states that parties should commit to ‘tackle false, misleading, misinformation or disinformation’. Again, this seems to be a repetitive statement amongst both the IHR amendments and the treaty itself. Art. 17(b) requires that WHO “member states” conduct “regular social listening and analysis” (aka surveillance) with the aim of counteracting and developing strategies to deal with misinformation. This not only gags freedom of speech, it also threatens scientific discourse and access to information. As Melissa Fleming, the UN’s Under-Secretary-General for Global Communications, stated during the 2022 WEF panel meeting: “We own the science, and we think that the world should know it”.
Descent into totalitarianism
To become international law, the amendments require simply that 50% of WHO “member states” approve them. The ‘Pandemic Treaty’, by contrast, requires support from two-thirds of the World Health Assembly (WHA), where each country, regardless of size, casts a single vote.
As might be expected, discussion about the import of these amendments is getting very little or no airplay in the mainstream media. Accordingly, there is no public debate or discussion to speak of going on, except in the realms of ‘alt media’ that is either not heard by the majority or, when it is, it is rapidly dismissed, as being the rantings of conspiracy theorists.
There is some limited pushback from a handful of daring and outspoken politicians, although some of the few who have spoken out have faced dire consequences. For example, not long after UK MP Andrew Bridgen presented his concerns to Parliament, he was permanently expelled from his party, in his case, ostensibly for comparing COVID-19 vaccines to the Holocaust.
Without an international uprising by the grassroots, these amendments will go ahead. Our silence and passivity are our consent. It is, without question, part of the slow descent into totalitarianism, taking us further and further away from principles and values that have characterised many civislisations over recent millennia, namely the right to liberty, the rights of the individual, and importance of national sovereignty.
What can we do to stop WHO supremacy over our health?
The starting point has to be communication and education. That means speaking up and speaking out. We have to open up conversations between the public, politicians, governments, world leaders, corporates, non-profits and influencers in their many and diverse forms. This subject needs to become daily conversation in households around the world, not just a topic of interest for the privileged few at the occasional dinner party.
We must give voice to those that have been up to the eyeballs with this issue for the last couple of years. Right up there is former IHR legal consultant, Dr Sylvia Behrendt, and senior scholar and former scientist at the WHO, Dr David Bell.
There then needs to be intensive public lobbying and discourse based on a proper understanding of these amendments and the proposed treaty, along with the implications they will have if left in their current form.
Timelines
Although the amendments and Treaty are not yet implemented, governments have been preparing ground and slowly easing us off into the changes. This year, between 20-24th of February, the Working Group on IHR (WGIHR) had its second meeting where the amendments were discussed for the first time. Next steps were agreed regarding more in-depth negotiations, which took place between 17-20th of April.
Following are a few additional dates for your diary:
- May 2023: 76th World Health Assembly. The meeting’s theme is “Saving lives, driving health for all” where WHA delegates, agencies and representatives will discuss ‘future priorities’. INB are preparing a progress report submitted ‘for consideration’.
- 12-16th June 2023: continuation of the meetings of the INB drafting group
- July 2023: 6th meeting of the INB and drafting group. Meeting of the WGIHR (4th meeting)
- September 2023: UN High-Level meeting on Pandemic Prevention, Preparedness and Response. This meeting seeks to ‘further mobilize political momentum’
- October 2023: 5th meeting of the WGIHR
The INB is to hold four further sessions early 2024 in preparation for the 77th WHA meeting in May 2024. At this assembly, the WHO will aim to adopt both the IHR and the Pandemic Treaty. If adopted (according to the WHO Constitution Art 19 for the treaty & 21 for the IHR Amendments), member states will have 10 months to submit reservations or reject the amendments/treaty. If no rejections or reservations are submitted, these will become binding law within 12 months (May 2025).
The treaty requires 30 countries to ratify it. The IHR amendments would come into force early 2025 only for the countries that do not issue a rejection.
Final thoughts
The UK, after Germany, remains the second largest country donor to the WHO in Europe (Fig. 2). UK citizens have already signed a petition asking for a referendum before the Government commits to signing the IHR amendments and the Treaty. After a debate in the UK Parliament on 17th of April 2023, the UK Government concluded that a referendum is unnecessary and that “the UK would remain in control of any future domestic decisions about national restrictions or other measures” [see the full response here]. Is this a reassuring statement or simply wilful blindness? The last two years and the binding nature of WHO’s supremacy over nation states would point to the latter.
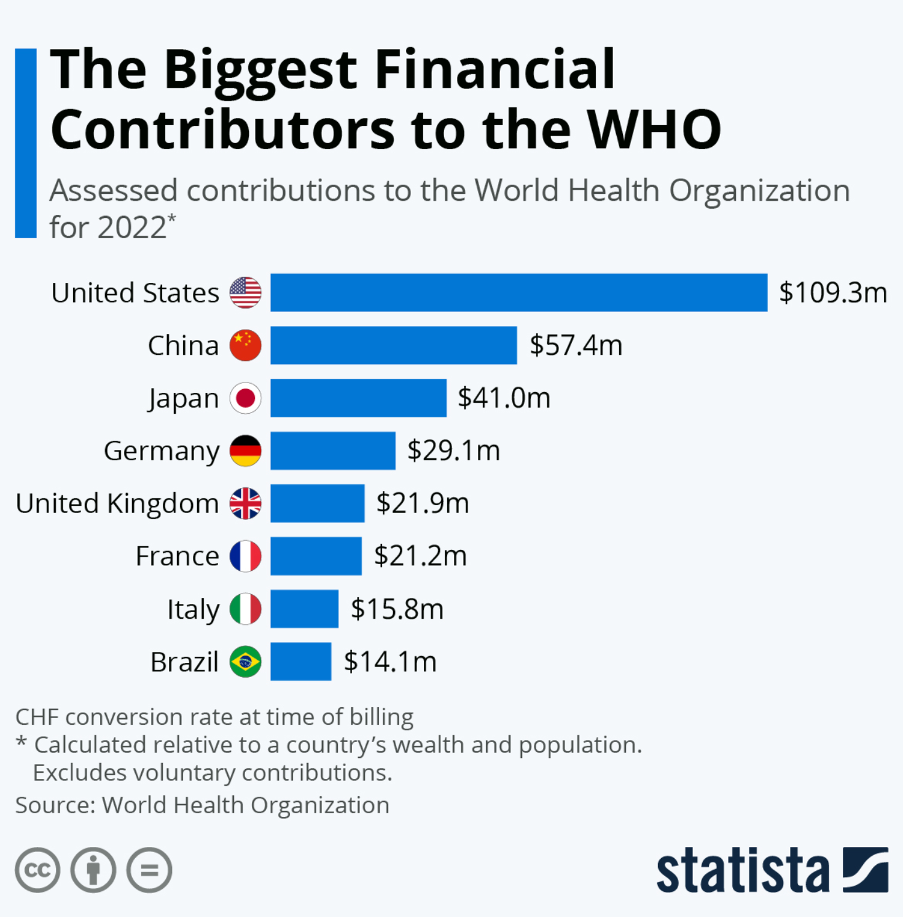
Figure 2: WHO member state contributions to the WHO in 2022. Source: Statista.
We, the public must recognise the risks of handing such power to an unaccountable and unelected, supranational organisation as the WHO, supported so strongly by vaccine interests and one that is now positioned as an investment opportunity. Countries have the right to reject as well as the right to exit the WHO – meaning there is still a way out before it’s too late. What happened to people’s desires to protect the rule of law, protect our inherent human rights, and our democracy? These are not privileges, they are rights.
The task ahead of us means blocking this process at the national level, in multiple countries. As outlined in the Declaration of Alma Ata Article IV – we have a right and duty to participate, individually and collectively, in the planning and implementation of our own health care.
Let’s do it.



0 Comments