


Why the Covid Vaccines Were Never Likely to Be Effective
by A Midwestern Doctor | Jun 5, 2022
I have successfully been fighting a drawn-out battle with multiple employers to avoid getting vaccinated (as have a few people I am very close to). Over the last few weeks, staffing shortages and customer absences have occurred at our employment sites due to everyone getting ill from COVID. This is particularly unusual given that this wave is happening during the summer (which is typically the time when respiratory viruses are at their lowest levels, something most likely linked to seasonal variations in vitamin D levels and levels of outdoor physical activity).
We have all noticed that most of the individuals who have gotten ill were vaccinated and had received their boosters. One of the predictions we regretfully made before the COVID vaccines entered the market was that the vaccination program would prevent the population from developing herd immunity to COVID-19 and thus indefinitely prolong the pandemic. A somewhat related parallel was the chicken pox vaccine (which had no real justification for being created) resulting in a permanent sustained increase of Shingles (a disease much worse than chickenpox) because the vaccinated populations lost their herd immunity to varicella zoster.
For those who remember, at the start of the pandemic, everyone predicted the virus would follow three waves like other famous respiratory viruses such as the 1918 Influenza. Presently we are experiencing a sixth wave of COVID-19, and private documents leaked to me by a colleague who works for the WHO suggest the WHO is planning for this pandemic to continue for years (that is the most I can share in order to protect the identity of the leaker).
Due to these events, I was requested to write an article on why the COVID vaccines were unlikely to be effective. With pharmaceutical products, I prefer to focus on their dangers rather than their ineffectiveness because being ineffective is typically less impactful than being toxic. This is a common thought process and has held true with discussions on the COVID vaccinations, where questions of their safety are discussed more often than questions of their efficacy. I believe shortcomings in their efficacy is critically important to discuss for two reasons:
•The basis for the mandates is predicated upon the vaccines being effective, particularly in the prevention of infection, and most importantly transmission.
• The refusal to consider other means for addressing the pandemic were based upon “increasing vaccination uptake“ being the best approach or addressing the pandemic.
Overview
Robert Mendelsohn made an excellent case that Western medicine has effectively usurped the role that the Church used to play in society (this is best detailed within Confessions of a Medical Heretic). There are many religious parallels, for example the ever present white coats serve the same role a priest’s robes held in the past. Vaccines likewise have assumed the role of a holy water or sacrament each convert of the religion must be baptized by and must never question (this was why within a recent article on medical gaslighting, I highlighted religiously orientated song lyrics that coincidentally described the experience of someone committing blasphemy by suggesting a medication could be harmful).
Because vaccines have assumed the role of a holy sacrament, when you attempt to discuss any issue with an injection, most doctors will default to “I believe vaccines were the most beneficial medical innovation ever invented” and in varying degrees turn hostile towards the injured patient who attempts to bring a vaccination side effect to their attention. The blind faith given to immunizations makes it extremely easy to market highly dubious or unproven claims about these products, because regardless of their absurdity, they are taken up as gospel by the medical profession. What has happened with the COVID vaccines is particular egregious, but all of it was based upon a century of building blind faith in these injections (for those wishing to learn more on this topic in the immediate future, Suzanne Humphries MD has done the an excellent job exposing it here).
At the time when the COVID vaccines were first being proposed, there were two major issues nearly everyone studying the issue was aware of:
•Despite decades of work, the Chinese government (and Western programs working in conjunction with the Chinese government) had not been able to develop a safe or effective vaccination for SARS-CoV-1. This is because SARS is a very difficult pathogen for which to make a safe and effective vaccination.
•It typically takes years to develop a new vaccination, and months to manufacturer it once a formulation has been decided upon.
On many levels, I think operation Warp Speed was a monumental achievement, and the clever design of it (best described by Peter Navarro) pulled off a variety of things many had thought were impossible. However, the individuals who ran Operation Warp Speed only appeared to understand the business aspect of the pharmaceutical development and not the medical aspect.
Typically elected officials defer questions of science to scientific experts within their administration. The only noteworthy exception I know of was Ron DeSantis, who (as detailed in Scott Atlas’s book) independently looked at the data and came up with a radically different (and highly successful) approach to addressing the pandemic (DeSantis’s approach mirrored the Great Barrington Declaration).
In my opinion, the lack of medical knowledge on vaccination within the Trump administration to a large extent invalidated Operation Warp Speed because at the end of the day there was no getting around the fact it was impossible for a somewhat safe and effective vaccine to be made in the short timeframe given to do so (a few individuals like Paul Alexander did attempt to bring attention to the medical issues but were ignored as everyone deferred to Fauci and Birx).
From having studied these industries (pharmaceutical, chemical, etc.) over the years, I have observed that whenever a not fully safe or effective product is brought to market, industry will bridge the gap in safety or efficacy through corrupt scientific studies, lobbying, lawsuits, marketing and public relations. This situation is analogous to one trying to fit a square peg through a circular hole, and opting to pound peg into the hole with a hammer rather than round off its corners when resistance to the product is encountered. I would argue this is also what happened with the COVID-19 vaccines.
When potential vaccinations were being evaluated, a variety of vaccination platforms were considered. Because the mRNA platform was best able to meet the needs of industry, it was the one that was ultimately settled upon (with recombinant adenovirus vector vaccine is being the second choice). There were however numerous serious issues in their design that scientists such as Mike Yeadon and Stephanie Seneff pointed out well before the vaccines entered the market. The predicted consequences of these design flaws have since proven themselves, so it is almost certain the manufacturers were also aware of these issues.
I was able to identify a few potential explanations for why badly designed vaccines were chosen:
•The chosen design represented the only possible way to get a product that could be approved onto the market in the short window of time before the pandemic ended. On a related note Fauci has been pushing for mRNA vaccines for years because they allow a much shorter turn around time from identifying a targeted antigen sequence to creating a mass produced vaccine for that sequence. This is especially necessary for a rapidly changing virus like influenza because it is nearly impossible to accurately predict what the dominant strain will be at the time traditional vaccines need to be made to be ready in time for the Flu season.
•Bringing mRNA technology to the forefront had the potential to rescue the pharmaceutical industry from the existential threat it was facing over its inability to develop new pharmaceutical drugs. There are so many applications of mRNA technology that it likely represents a multi-trillion dollar industry. To many this presumably justified taking advantage of the “emergency situation” to conduct the large-scale human experimentation necessary to develop the technology.
•Having a vaccine which selected for the propagation of variants (that the original vaccine did not work against) was a long-term business strategy to sell future vaccinations designed for those variants.
•Something more nefarious was in the works.
Once it became clear to me how bad the mRNA vaccines were going to be, I investigated what approaches were being pursued by countries outside the Western sphere of influence. Russia chose an adenovirus vaccination platform (like Johnson and Johnson and AstraZeneca), which could have either been due to safety concerns over the mRNA technology, nationalistic pride or an inability to produce the mRNA technology.
China however, despite receiving many solicitations for an mRNA vaccine, chose to avoid these newer spike protein production factories entirely, and instead went for a an inactivaed SARS-CoV-2 viral vaccine. While rarely publicized, China’s vaccine, which is used around the world has subsequently proven itself to be the most effective vaccination on the market.
Note: Cuba, India and Iran (despite spending much less money and having a more primitive vaccination development apparatus than the United States) have also developed alternatives to the spike protein producing vaccines. Cuba has developed a variety of protein subunit vaccines (this is what Novavax has been unsuccessfully trying to do since the start of the pandemic) while India and Iran, like China have used inactivated viruses.
This has often led me to wonder if the SARS-CoV-2 virus was deliberately designed by the Chinese military so that:
•It was a dangerous virus that was not be deadly enough to expose the Chinese government to an existential risk by releasing it
•The most likely vaccination to be developed in response to the virus (and expected to be mandated upon Western populations) would be highly dangerous.
Meeting both of these conditions in turn facilitated the creation of a stealth weapon to disable China’s adversaries. As China was collaborating with Fauci’s contingent to conduct covert gain of function research, the Chinese military was almost certainly aware of America’s biologic countermeasures technology. Given that a vaccination that rapidly produced SARS-CoV-2’s novel spike proteins in the blood is highly dangerous and it was reasonable to predict this would the most likely method of vaccination to be developed to SARS-CoV-2 (assuming you understood the full spectrum of vaccine countermeasures available), China’s complicity in this disaster is an interesting question to ponder.
Vaccination Trials
Educated professionals are taught a very specific way to interpret published research. This methodology results in it being very easy to trick these professionals because research papers can be crafted to emphasize the positive scientific qualities they are taught to look for and omit mentioning the critically important pieces of information they are not taught to look for. While this fundamental scientific literacy is never taught in medical schools, a variety of authors such as Drs. Malcolm Kendrick and Peter Gøtzsche have made this education available for those who seek it.
When the NEJM trial was published on 12/30/2020, much fanfare was made of the vaccination being “95% effective.“ This resulted in almost every physician I spoke with (both in person and an online groups) stating “well we knew the vaccination would be effective, but we never dreamed it would be this effective” (which in effect meant: “this is a modern day miracle and our salvation that will end the pandemic”). As a result, it was quite difficult to have critical evaluations of Pfizer’s study when discussing it with colleagues.
My spouse and I in turn had a variety of unsuccessful arguments with administrators over the Pfizer’s vaccination trial once it was published as we knew a mandate was coming. Our central arguments (most of which have since been proven true) were:
•The high-risk groups likely to have complications from the vaccine were mostly excluded from the study (ie. the elderly, the COVID recovered, and those with pre-existing autoimmune conditions).
•The trials did not test if the vaccines would reduce transmission or the asymptomatic spread of COVID.
•The reported rates of adverse events were 4-5 times greater than those reported for the influenza vaccination (59% verses 12-15%), which is highly unusual for a vaccination.
•The absolute benefit for the vaccination was very small; you had to vaccinate 119 individuals to prevent one minor case of COVID (versus 59% of recipients experience adverse reactions from the vaccine), 2711 to prevent one hospitalization, and well over 20000 to prevent one death (approximately 20,000 trial participants received the vaccination, which was too few to detect a reduction in mortality). This meant there was no proven mortality benefit from the vaccine.
•Critical long-term follow-up to determine the risk benefit ratio for these immunizations was not available and the Pfizer has refused to release their raw data for outside review until at least 2025.
Given the tendency of pharmaceutical companies to fudge and distort data, and my knowledge that numerous severe adverse reactions I had seen reported in Facebook groups by trial participants did not appear within Pfizer’s paper, I was relatively certain the vaccine would be unsafe and ineffective. Some of this analysis was possible due to pre-existing knowledge regarding the common issues with vaccination, and it is my belief that had physicians not been anchored to the “95% effective!” claim, most of the objections are mentioned above would have been self-evident from a critical evaluation of Pfizer’s paper.
I was never formally taught how to detect research fraud. Rather, it is a skill I picked up over the years by thinking critically about research papers I read in my free time. As such, I do not consider myself to be an expert in this regard.
Fortunately, Peter Doshi PhD is. Doshi serves as a senior editor for one of the five most prestigious medical journals in the world (the British Medical Journal) and was willing to break from the pack to discuss critical issues with the COVID vaccination trials. Doshi in turn did a deep dive on the available data and in a series of BMJ editorials, Doshi pointed out numerous red flags that were never discussed or addressed by the medical community.
On 10/21/2020 from analyzing the available trial protocols, long before the NEJM publication was available, Doshi accurately described how the design of these trials fundamentally could not fulfill the public promise the vaccines were being thoroughly evaluated for safety and efficacy. At the time, Doshi raised many of the same objections that later jumped out to me once I read Pfizer’s NEJM publication:
•Serious safety issues have occurred in the past with vaccinations that were inappropriately rushed to market for “pandemic” situations.
•The vaccine trials were only designed to assess for an improvement in minor disease related symptoms and not clinically meaningful outcomes like hospitalizations or deaths.
•The trials were not designed to assess for the ability of the vaccinations to stop transmission.
•The elderly and minorities, both groups who were expected to face significant pressure to be vaccinated, have significantly different risk-benefit profiles from vaccination than the general population, but were not being sufficiently enrolled in the studies.
On 1/4/2021, shortly after the publication of Pfizer’s vaccine trial in the NEJM, Doshi posted an editorial that cited information made available in the FDA’s report on Pfizer’s trial which noted the following:
•While much fanfare has been given to the fact the placebo group developed 162 cases of PCR confirmed COVID and the vaccine group developed 8 cases (resulting in a “95% efficacy” for the vaccine), there were also “3410 total cases of suspected, but unconfirmed COVID-19 in the overall study population, 1594 of which occurred in the vaccine group vs. 1816 in the placebo group.” This was only possible to later discover from the FDA’s report and was never mentioned by the NEJM.
•More participants were excluded from the study for undisclosed reasons than were used to make the case for “95% vaccine efficacy.” 371 individuals were excluded from Pfizer’s efficacy analysis for “important protocol deviations on or prior to 7 days after Dose 2,” of which 311 were from the vaccine group vs and 60 from placebo.
•Both of these raise major concerns on the actual efficacy for the vaccine. For example, when the unconfirmed cases were included, Doshi calculated the vaccine was likely between 19% to 29% effective and hence failed to meet the minimum standards (a 50% efficacy) for approval. Unfortunately, the top 5 medical journals (with the exception of the BMJ) have abjectly failed in their responsibility to inform the public of this critical information. The fact that the NEJM failed to disclose any of this is a testament to how corrupt the scientific publication industry has become.
•The higher use of fever medications in the vaccine arm suggested the trial was not blinded and the minor COVID-19 symptoms being assessed for (such as fevers) may have been concealed with these medications.
•These data irregularities have made it critical for Pfizer and Moderna to make their trial data available to the public, which they so far have adamantly refused to do.
On 5/18/2021, Doshi made the case that insufficient data was available for a regulatory approval: the necessary long-term follow up studies were ether not being conducted or were years from completion and no bio-distribution data for the vaccines were available. At this time, the BMJ asked the vaccine manufacturers how they would reconcile these critical gaps in knowledge with seeking a formal drug approval. Each company was evasive and refused to answer if they were seeking FDA approval, but three months later on 8/23/21, Pfizer received an FDA approval for their vaccine.
In a clever act of legal subterfuge, Pfizer’s vaccine was then transformed to Schrödinger’s cat. By being approved but never being made available in the USA, it received the legal weight of an FDA approval without the reciprocal liability for an FDA approved product, allowing Schrödinger’s vaccine to be FDA approved when convenient and only emergency use authorized when convenient. This approval forced numerous friends in the military who did not want the vaccine to be forced to receive it, some of whom are now disabled but have no recourse for their injury because the product they received was not FDA approved.
On 8/23/21 immediately preceding the approval of Pfizer’s vaccine, Doshi used the now available data from the approval to highlight serious issues with a potential FDA approval:
•The FDA was refusing to provide transparency in their approval process or hold an open hearing on Pfizer’s vaccine prior to approving it.
•Data after 6 months of follow-up was being deliberately withheld by Pfizer (the original trial was supposed to last for years).
•There were now numerous data sets showing that the efficacy of Pfizer’s vaccine significantly declines over time. For example, by early July, Israel had reported Pfizer’s vaccine efficacy had dropped from 95% to 64%, and by late July and fallen into 39% (thereby missing the 50% efficacy mark).
•There is good reason to suspect Pfizer terminated their trial early to conceal the waning immunity that was occurring.
•At six months, only 7% of those who are enrolled in the trial remain blinded. This once again cast serious doubts on the validity of Pfizer’s data and also made it impossible to evaluate delayed reactions or chronic illness arising from the vaccinations.
•As the vaccines were failing in their initial promises, the goal posts were moved to preventing serious injury and death. This, as discussed Doshi’s initial 10/21/2020 editorial was something the trials were never designed to test for, despite individuals such as Scott Gottleib trying to revise history by claiming the trials did (others like Fauci were equally duplicitous, claiming on television they would while admitting in scientific publications they would not).
Note: moving goal posts is very common in vaccination campaigns once the unrealistic promises sold to the public to get them behind the campaign fail to materialize.
•In their final publication while Pfizer and Moderna claimed to have demonstrated vaccine efficacy against “severe disease”, neither gave the information necessary to substantiate what constituted “severe disease.” Fortunately, they did provide information indicating the classification was being used inappropriately.
-Pfizer did not disclose the number of COVID-19 hospitalizations that occurred, but did disclose 0 COVID-19 deaths occurred.
-Moderna admitted only 9 of their 30 cases of “severe” COVID-19 were even hospitalized. Within Moderna’s trial, 3 COVID-19 related deaths occurred; 1 in the vaccine group and 2 placebo (which is resulted in it being labeled as 50% effective against preventing death, despite this figure being based on a single additional death). Additionally 15 of those vaccinated died, while 14 who were unvaccinated died.
Note: I personally believe the claims of the vaccination being 100% effective for preventing all hospitalizations and deaths are false as I know numerous vaccinated individuals who were hospitalized for COVID-19 and I know of an anti-mandate group that filed charges against a county health department for claiming the county’s severe COVID cases were arising in the unvaccinated despite verified evidence proving otherwise. Likewise, numerous international datasets, such as this one discovered by Steve Kirsch and this compilation by Robert Clark suggest vaccination not only fail to prevent hospitalization but actually increases the risk of hospitalization. In my experience, when absolutist claims are given to dismiss dissenting views (as they often emotionally appeal to the masses), these claims are generally fraudulent because it is exceedingly rare to ever have anything result in a 100% outcome either way.
On 11/2/21 an investigative journalist working for the BMJ published an article corroborating a Texas whistleblower’s accusations of data fraud in Pfizer’s vaccine trials. Some of these accusations were later confirmed at another major trial site for Pfizer in Argentina (for example by this research subject). There are a few key points relative to Doshi’s editorials that were confirmed by the whistleblower testimony:
•The trial was effectively unblinded, meaning the minuscule benefit detected from Pfizer’s vaccination could likely be attributed either to the placebo effect or biased investigators choosing not to diagnose COVID-19 in the vaccinated test subjects.
•Many significant adverse events in those vaccinated that were not followed up on or recorded.
•This single whistleblower over her two weeks of employment witnessed numerous instances of individuals with COVID-19 like symptoms not being tested for COVID-19 (the testing site in fact lacked the capacity to conduct sufficient PCR testing). Given that Pfizer’s 95% efficacy was based upon “162 cases of PCR confirmed COVID in the placebo group while the vaccine group developed 8 cases” it is entirely possible this whistleblower alone (had she not been fired) would have witnessed enough cases of COVID-19 developing in the vaccinated cohort to bring the efficacy of Pfizer’s vaccine below 50% .
•Other employees at the trial site report at similar concerns, but for fear of losing future job prospects (this is what always happens to whistleblowers in the pharmaceutical industry), they only spoke to the BMJ on the condition of anonymity. One for example described an environment at the trial site unlike any she had experienced in her 20 year career as a clinical researcher.
•The whistleblower repeatedly tried to bring attention to her superiors regarding the serious data integrity breaches occurring at the site. They repeatedly refused to address the issue, so she complained to the FDA. The FDA likewise did absolutely nothing address the issue but rather informed the whistleblower’s superiors, who promptly fired her. Ultimately, the FDA only inspected 9 of Pfizer’s 150 the trial sites and 1 of Moderna’s 99 trial sites; as you might guess the Texas site in question was not inspected by the FDA which raises serious questions over what had to have happened to trigger the inspections that did happen.
Note: All of this initially appears unbelievable, but as detailed in the previous article discussing 30 years of the FDA working diligently to cover up significant harms from anti-depressants, there is a past precedent for this malfeasance. Pfizer also continued to use this research vendor indicating they likewise had no real objections to their conduct. Members of the FDA responsible for evaluating these sites spoke on record immediately prior to Operation Warp Speed’s first vaccine being approved saying critical oversight from the agency would not occur, but what occurred was far beyond what any of us expected.
Within hours of the BMJ publishing this article, Facebook moved to censor it. Giving the prestige and credibility of the BMJ, even by the current rules of “authoritative sources,“ this was excessive, and before the day was over, the BMJ had published an open editorial to Mark Zuckerberg chastising his company’s behavior.
On 12/23/21 Doshi penned an editorial that noted that while a variety of additional research trials were legally required in return for receiving an EUA (Pfizer agreed to do 13 and Moderna 8), many had not been done, and basic pieces of information such as the study protocols were only available for 5 of Pfizer’s studies and 5 for Moderna. Most of the protocols that were available were only available because to the European Medical Agency legally required them to be visible, something the more corrupt FDA does not require a pharmaceutical companies to do.
On 1/19/22, Doshi published an editorial once again emphasizing the critical importance of raw data being made available to the public and noted Moderna, Pfizer and AstraZeneca were all refusing to release the raw data for their EUA vaccines (as was Regeneron for their monoclonal antibody therapy). The FDA likewise refused to make this information available, but fortunately lost in court and was forced to disclose Pfizer’s vaccine data, which has resulted in the Pfizer papers that are now being brought to the attention of the public.
My heart goes out to Peter Doshi. I can only begin to imagine how frustrating this entire process has been for him. He even told the FDA his proven concerns at an advisory meeting (which can be watched here) and was completely ignored by the agency.
Surrogate Markers
Frequently in research, it takes a significant amount of resources to quantify the meaningful physiologic changes that occur in research subjects. One solution the pharmaceutical industry has found to this problem is using “surrogate markers.”
The idea behind surrogate markers is that if it is known that something is “good” for you, such as lowering blood pressure, then it can be assumed that if a pharmaceutical is observed to create that “good” effect, it can also be assumed that the pharmaceutical will improve the health of the participants. This idea often does not hold up, and pharmaceuticals that are proven to improve a surrogate marker often end up having negative rather than positive affect on recipients. For those interested in learning more about the problems with surrogate markers, Malcolm Kendrick has extensively detailed in Doctoring Data how surrogate markers ruin clinical research.
With vaccinations, their primary surrogate marker is the production of antibodies to the target antigen. Because of this, vaccination designers often develop tunnel vision towards ensuring sufficient production of the necessary antibody. In certain cases, this becomes highly problematic. For example, with the HPV vaccine, Merck discovered that it was quite difficult to produce sufficient antibodies there, so to solve the problem, they used a very strong adjuvant that also has a side effect of creating a variety of autoimmune conditions and has resulted in their vaccine being much more likely to harm than benefit the recipients.
Many of the doctors I spoke to about the COVID-19 vaccinations would not budge on their position that the vaccination reducing symptoms meant that it would also reduce the transmission of COVID-19. This has since been proven false and illustrates the incorrect application of a surrogate marker (reduction of minor PCR confirmed symptoms) to a meaningful clinical outcome (reduced transmission of COVID-19).
The Covid vaccinations were designed to maximize the production of antibodies to the virus, and from what I have been able to piece together from reading the literature, antibodies to the spike proteins were found to be the easiest to produce which likely influenced spike protein producing vaccines being decided upon. Unfortunately, there are many components to the immune system beyond antibodies to a specific antigen, and in many cases when production of a specific antibody is prioritized, the net result is impaired rather than improved immunity.
Important measures of efficacy such as T and B-cell function and NKC activity are technically much more difficult, expensive, and time-consuming to measure than antibody levels. From reading Pfizer’s leaked EMA documents (I have some experience with drug development applications) many studies that would typically be required for a new drug application were waived, and Pfizer as a result did not complete them, which is likely why testing comprehensive measures of immunologic function was also skipped.
Immune Changes from Vaccination
Immunology is often referred to as the last frontier of medicine because so much remains unknown about the immune system. I personally believe the discipline of immunology has been heavily distorted by the desire to develop vaccinations (and other immune therapies), which has resulted in the immune system being viewed through a pharmaceutical production lens rather than a broad view of the entire system.
One of the largest shortfalls of this approach is that when we attempt to artificially alter the immune system with vaccinations without first understanding how the immune system actually works, there are often a large number of unintended consequences. For those interested in understanding the subject further, Miller’s Critical Review of Vaccination Studies is the best compilation I have come across of literature demonstrating common side effects resulting from immune dysregulation due to vaccination.
Efficacy was continually chosen over safety when designing the mRNA vaccines (as there was a very limited window to get them to market). Two things done to make sure the vaccines would “work“ were to substitute pseudouridine for the uridine in the mRNA so that it resisted being broken down (thereby making it able to produce proteins for a longer period of time), and codon optimization, which was done to increase the translation and synthesis of the synthetic mRNA.
These created many potential issues, including a very long half-life for the synthetic mRNA. Not surprisingly, data on the persistence of the mRNA was never made available to the public. A few months ago, a study was published showing the mRNA persists for at least 60 days, and another was published a year ago which showed the mRNA vaccine produces a prolonged robust humoral response (which unfortunately can often create autoimmunity).
An introductory principle in immunology is that there is a constant balance between the Th1 (cell mediated or cytotoxic) immune response and the Th2 (humoral or antibody) immune response as the Th1 response releases IFN-γ which effectively suppresses the Th2 response, and the Th2 response releases IL-4 and and IL-13, both of which effectively suppress the Th1 response. The Th1 response tends to be excellent at dealing with intercellular pathogens and cancers, while the Th2 response tends to be excellent at dealing with pathogenic substances such as toxoids, parasites and encapsulated bacteria that are outside cells or on their surfaces. The balance between Th1 and Th2 is frequently discussed within the hygiene hypothesis, which posits many of our chronic diseases arise from an imbalance between these two systems due to modern sterile living conditions.
Classical vaccinations (those with an antigen and adjuvant such as aluminum) tend to excessively increase the Th2 response. Likewise, there are a variety of effective conventional and alternative medical therapies that elevate the Th1 response and suppress the Th2 response which are often used to treat complications from vaccinations, cancers or viral infections.
It is clear the vaccines are producing significant alternations in the immune response, although conflicting evidence exists regarding the nature of that alteration. One subject of debate amongst my colleagues (including knowledgeable immunologists) is if the mRNA vaccines are excessively increasing the Th2 response and reciprocally weakening the Th1 response. This is in line with previous vaccinations and would explain many of the effects seen with the vaccinations, but since there is ample evidence that supports this hypothesis and ample evidence that refutes it, I cannot take a position on it.
Senef for example shows that while natural COVID infections stimulate a Type 1 and Type 2 INF response (IFN-γ), the COVID vaccinations appear to suppress both of these responses, which potentially explains the increased susceptibility to viruses experienced in vaccine recipients (shingles is a common side effect of the mRNA vaccines). Senef hypothesizes this may be partly due to pseudouridine being incorporated into the mRNA vaccines, which was done to suppress the innate immune response to the synthetic mRNA and hence protect the mRNA product from being broken down. This may also have the unintended consequence of creating prolonged suppression of the immune system that goes far beyond inhibiting the breakdown of foreign mRNA. It is also possible this immune suppression is due to the lipid nanoparticles themselves that are used to deliver the mRNA to cells, as these particles are far from biologically inert.
I have also read verified reports of individuals developing AIDS defining illnesses of immunosuppression immediately following vaccination, which also happened to the uncle of a good friend of mine. While severe immune suppression can occasionally occur from the vaccinations, typically the immune suppression comes later and is more subtle and difficult to recognize.
The specific immune alterations that occur from mRNA vaccination is a lengthy topic beyond the scope of this article. For those interested, this is one of the most detailed papers I have read so far discussing the alterations in the immune response created by the mRNA vaccinations. Regardless of the mechanism however, my current hypothesis is that these pathologic alternations in immune response are likely a consequence of the prolonged immune response to persistent mRNA products within the body.
Original Antigenic Sin
A few months ago, data suggesting increase susceptibility to illness in the vaccinated population like this presentation from Walgreens surfaced:
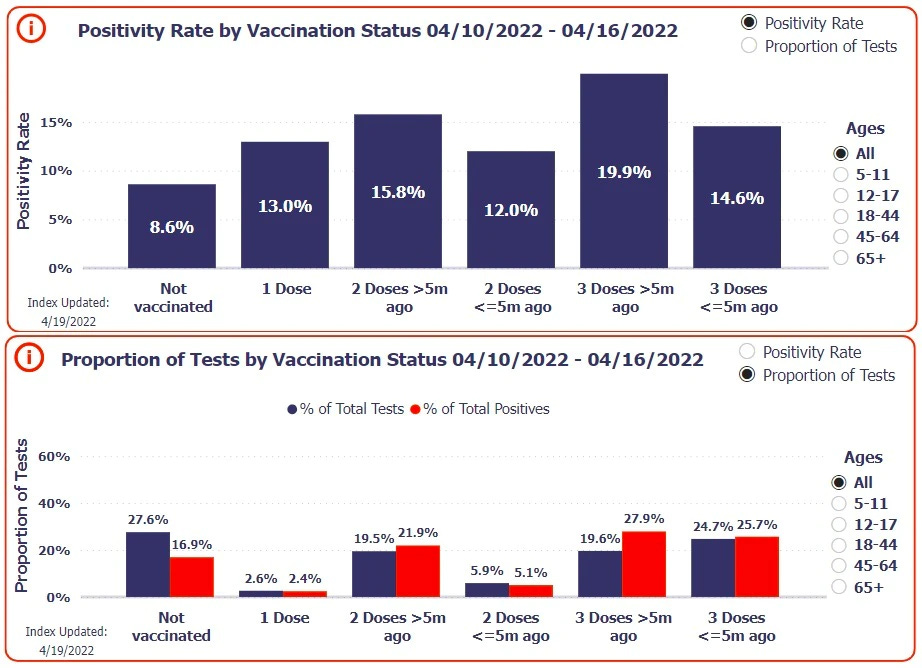
I have looked at many models to explain the unusual immune changes witnessed from mRNA vaccination (such as antibody dependent enhancement). So far the best model I have come across to explain the changes is known as Original Antigenic Sin (OAS). OAS postulates that the immune system has a finite ability to adapt to pathogens, and as a result, if an immune response is developed to one pathogen, the adaptive immune system’s ability to respond to other pathogens or variants of the original pathogen decreases.
To this point, data has now emerged showing mRNA vaccination impairs the ability of the immune system to develop immunity to new COVID variants as multiple components of the immune response necessary to mount this response appear to show impairment. This has most been directly shown in vaccinated individuals who are 5 times less likely to develop antibodies to the nucleocapsid of SARS-CoV-2 (which is needed to develop permanent immunity to COVID-19) than unvaccinated people. As detailed by Igor Chutov, Moderna (and almost certainly Pfizer) was aware of this early in their research and did something quite horrific by failing to publicly disclose this fact.
Because of OAS, more vaccines are not always better, and there have been multiple instances, such as in veterans immediately before the Gulf War, where simultaneous injection of multiple vaccinations was ultimately immunosuppressive for the recipients. Unfortunately, due to the blind faith given to vaccinations, the potential issue with the simultaneous administration of multiple vaccinations is almost never considered, and physicians who advocate deviating from the CDC schedule by spacing out vaccinations are met with open hostility (or worse) from the medical community. This is a shame because spacing out immunizations often significantly decreases the likelihood of a significant adverse event from vaccination.
Most of the evidence documenting the occurrence of OAS has been done with influenza vaccinations, as these typically increase your likelihood of developing a variety of other viral respiratory infections including coronaviruses and with strains of influenza differing from that contained within that year’s influenza vaccination. This effect is frequently observed the year following vaccination, and it is always ignored by flu vaccination advocates who believe the solution to all the world’s problems is to vaccinate as many people as possible. For those of you who would like to know more about the evidence for OAS, this article by the Children’s Health Defense Fund contains numerous studies that confirm the occurrence of OAS from influenza vaccination.
During the Italian COVID-19 outbreak I was informed by doctors in the area that patients who had received that years influenza vaccination were both more susceptible to COVID-19 and much harder to treat. After publishing this article, Vinu Arumugham kindly alerted me to this study and this dataset that show a significant association between Influenza vaccination and increased severity of COVID-19 outcomes. Given how frequently “get your flu shot” was the main piece of advice given for addressing COVID prior to the vaccinations being made available, the fact that it did the opposite is quite infuriating.
Promotion of Variants
Anytime something is introduced to eliminate pathogens, its introduction will inevitably create a selective pressure for the pathogen to evolve a resistance to the intervention. While I have never heard it described in this manner, this is how I make sense of the concept:
•The most difficult to evolve form of resistance is the synthesis of a new protein or enzyme created to neutralize the antimicrobial agent. Bacteria synthesizing an enzyme to prevent penicillin from destroying their cell wall is one such example.
•The second most difficult form of resistance to evolve is changing an enzyme’s receptor site so that an antimicrobial agent no longer affects it, while doing so in a way that also maintains the critical function of the receptor site.
•The easiest form of resistance to evolve is slightly changing the proteins sequence of an antigen (which continually occurs during replication of pathogens) to one that differs from the sequence the vaccination was designed to recognize. RNA viruses, such as SARS-CoV-2 are particularly prone to developing this type of resistance due to how rapidly they change during replication cycles.
It is commonly recognized that antibiotics promote the development of antibiotic resistant bacteria, but it is much less recognized that vaccinations produce the development of vaccination resistant variants. In my own assessment, some vaccinations are effective while many others are not. Typically, the vaccinations that are effective tend to promote a selective pressure that soon results in the vaccine no longer being effective. One of the best known (but not the only) examples of this concept is the pneumococcal vaccination, which over the years has continually needed to be updated with more and more antigenic sequences being included in the vaccine because Streptococcus pneumoniae developed resistance to many of the original vaccine antigens.
Another frequently under appreciated aspect of this process is the variants produced through a selective pressure tend to be more pathogenic than the original variants. This has been repeatedly demonstrated with both antibiotics and vaccinations (Miller’s references numerous published studies showing this occurs from a variety of vaccinations).
In order to prevent the creation of variants, two things are necessary:
•The vaccine must be effective enough to provide sterilizing immunity (this differs from immunity that improve symptoms but allows you to remain infected with the pathogen, which overtime can then evolve immunity to the vaccine).
•The vaccination must contain numerous antigenic sequences, as this makes it much more difficult for a pathogen to evolve resistance to the vaccination because even if one or two of its antigens spontaneously mutate a resistance to the vaccination, the pathogen will still be eliminated due to its remaining antigens being susceptible to the vaccination produced immunity. Ideally some of these antigens should be on conservative regions of the pathogen (such as the nucleocapsid) which are less likely to mutate rather than a rapidly changing region like the spike protein.
Most vaccinations tend to have a limited number of antigens because each antigen is expensive and costly to produce. The one exception are live attenuated vaccinations (which, with the exception of tuberculosis, are all viral vaccines) or killed vaccines, as by being pseudo-clones of the pathogen they also contain the wide range of antigens found on the target pathogen.
In summary, this all leads to the unfortunate situation where vaccinations often promote the evolution of a variant that through OAS, the immune system partially loses its ability to respond to.
The spike protein-based vaccinations have resulted in numerous variants evolving with different spike proteins that are resistant to vaccination induced immunity. This is particularly problematic because as discussed before the prolonged immune response created by the sustained production of spike protein “locks“ the immune system into targeting the no-longer present original variant rather than the nucleocapsid of the virus. Conversely, the Chinese vaccine does not suffer from this issue as it targets so many different antigens (including parts of the virus that are less likely to mutate) the virus has been unable to evolve a resistance to the immunity from that vaccine.
It is hence understandable why many doctors and scientists have publicly questioned the wisdom of mandating a vaccination for a virus that no longer exists. What I personally find perplexing was the FDA viewing the fact that the monoclonal antibodies that target a no longer existing spike protein as a suitable justification for pulling them from the market, but this same issue has not resulted in even an inkling of them changing their current vaccination recommendations.
The monoclonal antibody decision was particularly tragic because it was one of the few therapies that appeared to help vaccine injured patients. When the FDA withdrew it from the market, most of the existing stockpiles were immediately disposed of (one of my colleagues was able to rescue part of his hospital’s supply as it was being thrown away).
Influenza Vaccinations
In my own medical career, I have noticed that every single patient I have ever seen who ended up in the ICU for influenza had been vaccinated that same year. I have asked colleagues this question, and those who are open to vaccinations being harmful have reported the same observation. When I have looked at literature attempting to answer this question, I have found that influenza vaccinations do not appear to have any effect on hospitalizations from influenza (which argues against the value of these injections but also suggests my observations may overestimate this phenomena).
When the topic of influenza vaccination and hospitalizations is discussed, I often observe the incorrect application of surrogate markers. Doctors will typically assert individuals being in the hospital for influenza is proof everyone needs to be vaccinated, and whenever it is mentioned that the hospitalized patient was vaccinated, this glaring contradiction is rationalized as “well the infection would have been much worse if they had not been vaccinated,“ something we have likewise heard all too many times with the COVID vaccines.
Similarly, as far as I know, in every year where I’ve paid attention to it, we picked the “wrong” flu vaccine strain for the annual vaccination campaign. In bad influenza years with increased influenza hospitalizations, the surge is attributed to the wrong vaccination strain being chosen, but at the same time (because people always want to have their cake and eat it), it is always argued that the vaccine greatly mitigated the disease, and had we not vaccinated everyone, things would have been even worse, so it is therefore imperative everyone vaccinate against the flu.
Honestly resolving situations like this is why evidence based medicine is so important. Unfortunately, because medicine is also a political institution, evidence that challenges existing dogmas is often not considered when evaluating critically important medical policies.
Alex Berenson recently published an article that perfectly encapsulates my experience working with influenza patients. Briefly, in 1980 approximately 12 million influenza vaccinations were given annually within the United States. Come 2020, nearly 200 million influenza vaccinations were given. Despite this, there has been no impact on mortality from influenza. None at all.

I am hence quite worried that a similar situation to that show in this graph will arise with the Covid vaccinations unless the American people collectively put their foot down on all of this. Given the suppression of permanent immunity that has been created from the mRNA vaccinations, I unfortunately suspect this future is quite probable.
There are many metaphors that have been used throughout history to describe the tendency to fanatically cling to something that is clearly not working. I have used many of these metaphors in the past, and at this point I view situations like the fixation with annual influenza vaccination as examples of collective karma manifesting itself throughout a society.
After publishing this article, I was alerted to an excellent point raised by Robert Malone. Many vaccination production facilities cannot pause production without shutting down for a prolonged period, so to some extent the primary purpose of the annual influenza campaigns is to maintain the vaccine manufacturing capacity of these plants.
Regions of Immunity
As we conclude this article, we should also consider the potential impacts of vaccination on transmission (this has been the primary ethical argument for why it is necessary to violate individuals free will to vaccinate). As you may remember, it was initially claimed that the mRNA vaccines would prevent transmission (even though there was no clinical evidence showing the vaccines did this), and like many other lies, it has now been clearly proven that the vaccines do not prevent transmission. Like many other immunological concepts discussed in this article, this was entirely predictable from the design of the vaccinations. There is also some past precedent for other vaccinations, such as influenza and pertussis increasing. rather than decreasing transmission.
The route of exposure to a pathogen has a significant influence on the eventual type of immunity which is developed to the pathogen (this is a frequently discussed topic in holistic medical systems that often advocate against bypassing the normal routes of exposure to a disease). Mucosal immunity for example (which is mediated by a different type of antibody than that found in the bloodstream) is produced when a pathogen contacts the nasal or respiratory mucosa, but is not produced if an antigen bypasses the respiratory tract through a direct injection into the bloodstream.
This is why intranasal influenza vaccines produce a different immunity than intramuscularly injected influenza injections. This is also why Bill Gates, seeking to address the transmission issue, has been actively discussing making an intranasal COVID vaccination.
One rarely appreciated aspect of COVID-19 (particularly for the newer variants) is that the virus replicates in the nose, sinuses, and throat for a prolonged period of time and then eventually makes it to the lungs where it transforms into a serious infection. For this reason, if you administer a disinfecting agent to these areas early in the course of the disease, that is often sufficient to fully resolve the illness (I have tried this, it works).
The primary benefit of the COVID-19 vaccination being introduced to the bloodstream is that it reduces the likelihood you will develop symptoms from the virus being within your bloodstream. As those symptoms can be fatal, there is an understandable justification for wanting to develop immunity at this level. However, since the virus initially replicates within and spreads from your upper airway, the present form of vaccination is unlikely to affect your tendency to transmit, and you run the risk of becoming an asymptomatic transmitter of the virus since your symptoms are reduced by the vaccination.
To some extent, there is a past precedent with all of this from the pertussis vaccination (also discussed in Miller’s). This vaccination does not produce immunity to the bacteria, rather it produces immunity to the toxin the bacteria produces which causes whooping cough. As a result, many individuals infected with pertussis become asymptomatic spreaders of pertussis, and while it is not reported in the media, pertussis outbreaks often occur within vaccinated populations.
Conclusion
In my own opinion, one of the largest issues with “Science” in the current era is the very few people actually take the time to read scientific papers and think through what they mean. Instead, they depend upon the judgment of a “trusted expert” to analyze the paper for them. In many cases, these experts erroneously evaluate the literature.
One of the most frequent and disheartening examples of this phenomenon is how commonly the results within a scientific paper directly contradict the paper summary and conclusion. This is disheartening because most individuals who appraise scientific articles only read the introduction and conclusion, commonly leading them to reach an erroneous interpretation of the paper (in most cases a paper’s conclusions are more biased than the data contained within it to suppor the existing scientific orthodoxy).
It will hence be interesting to see how long the questionable policies we are following will prolong the pandemic and how future medical journals will evaluate the approach we took. In this article without going too deeply into the immunology, I have attempted to illustrate why I believe the current wave of COVID-19 we are seeing in the vaccinated is a direct result of chronic immune suppression from repeated mRNA vaccination. Like many, I am worried many of these individuals will eventually end up on a treadmill of indefinite vaccinations in an attempt to compensate for their diminished immune function.
Lastly, in the spirit of considering hypothesis alternative to my own, I will also note that some of my colleagues believe the current wave of COVID-19 is at least partly due to two antivirals were recently introduced to the market, Paxlovid and Lagevrio (both were FDA approved in late of 2021). The evidence for this theory is tentative at best, and may simply be a result of boosted individuals being more likely to request these medications.
Briefly, we have noticed patients taking Pfizer’s Paxlovid appears to have greater illness from this variant, which may be a consequence of the drug having a similar profile to HIV medications that are already known to cause immune suppression. To support this point, Pavloxid’s Israeli trial data shows individuals aged 40-64 who take Paxlovid become more likely to become ill if they were also fully vaccinated. The data is striking and I am presently at a loss for a mechanism that would explain this.
Merck’s drug is less frequently used (hence our clinical observations are quite limited), but it has a potentially harmful mechanism of action. To quote Wikipedia: “Molnupiravir inhibits viral reproduction by promoting widespread mutations in the replication of viral RNA by RNA-directed RNA polymerase.“ There have been widespread concerns this mutagenic process could result in either birth defects, cancers or the production of harmful variants or human cancers.
Given that there are already affordable and effective antiviral therapies for COVID-19 such as Ivermectin which do not have these safety issues, the current generation of “approved” COVID treatments again highlights the issue with a drug approval system that prioritizes profitable pharmaceuticals.
Thank you again for taking the time to read this and your support in sharing this content with individuals you believe can benefit from it.
Postscript: After writing this, I discovered Igor Chutov also noticed this surge in the boosted and was drafting an article an article at the same time I was on this topic. At the start of the COVID vaccination campaigns, national datasets emerged showing COVID vaccination was consistently followed by a spike in COVID-19 and videos of this trend were made (ie. this one). The new variant has provided further support of this hypotheses because now similar countries with dramatically different COVID vaccination rates can be compared to monitor their responses to this variant. The datasets Igor has compiled mirror what we have all been witnessing at our locations of employment and can be viewed below.


0 Comments