


The modified spike protein is dangerous and for very specific reasons.
by Jessica Rose | Jun13, 2022
There’s an article that was published yesterday (June 12, 2022) with the typical sensational headlines (that I loathe) to entice readers, but it is confirmatory, with images, of the amyloidogenic and possible prion-ability of modified mRNA spike peptides. It has a lot of ‘pretty’ pictures and confirms that the structures inducing arterial embolisms in post-injected individuals are not blood clots. These people were dead before they were embalmed, don’t worry.
Unlike normal clots which are gelatinous, almost jelly-like, these so-called “clots” contain extremely large, complex, repeating structural elements (all shown below) that are clearly being constructed in the blood of the victims who died from these clots.
Here’s a photo of a sample of these structures that were extracted from individuals who had passed within the past 4 hours (not the result of post-mortem blood stasis) by an experienced embalmer.

Here’s a vial of these raw clots, washed [free] of blood and preserved, before staining. These structures that were evacuated from inside blood vessels during embalming procedures within hours of death.
Before I share some of the weird images posted in this article, I need to do some scaling. Just, because, I like scaling. A blood vessel can change its inner diameter via vasoconstriction (see RAAS) but it would be safe to say, that for any selected blood vessel, the diameter would be somewhere between between 8 um-25 mm, depending on what type you pick and if its vasoconstricted.

So let’s assume our white lengthy, stringy bits in the above glass sample vial were extracted from 4 mm arteries. That seems about right, yes? So, I am not an embalmer, but I hear that clots ‘normally’ show up in veins and not so much in arteries. By the way, when a vein is blocked from a clot, this is called a venous thrombosis is and when an artery is blocked by a clot, this is called an arterial thrombosis. Is it a thrombotic bus or an embolic bus, House MD would ask? Well I would say these people died suddenly from arterial embolisms caused by these fibrous structures. The following photo shows what a gelatinous, ‘normal’ blood clot looks like in a big artery (heart-proximal?). It looks exactly like red current jelly.

Arterial Embolism. Causes, symptoms, treatment Arterial Embolism
So, now us non-embalmer laymen can rest assured that these strange white fibrous proteinacious structures are not blood clots. The structures did, however, obstruct the flow of blood in the arteries of these individuals and likely is what killed them.
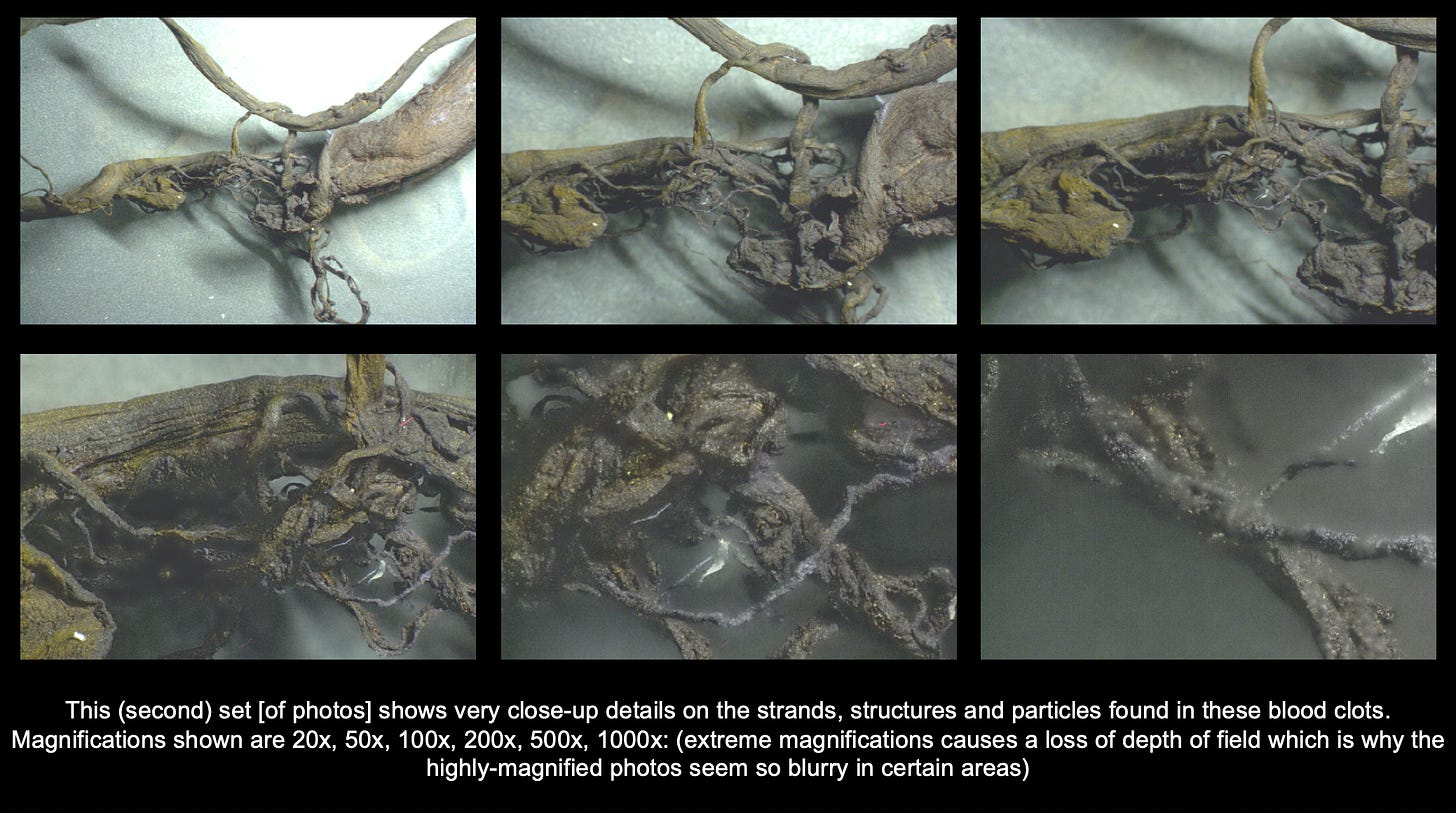
This first set [of photos] shows strange crystal-like structures that resist staining techniques and appear to show some sort of nano-scale, clear crystalline structures which would normally never appear in blood or blood clots.

Analyzed “blood clot” samples at 500X magnification.
Take a look at this increasingly magnified set of photos from photo set 2. Take note that since the larger diameter of these sample arteries is likely 4 mm, then the width of the shiny object is likely close to 0.1-0.5 mm, by my eyeball guess? What do you guys think?
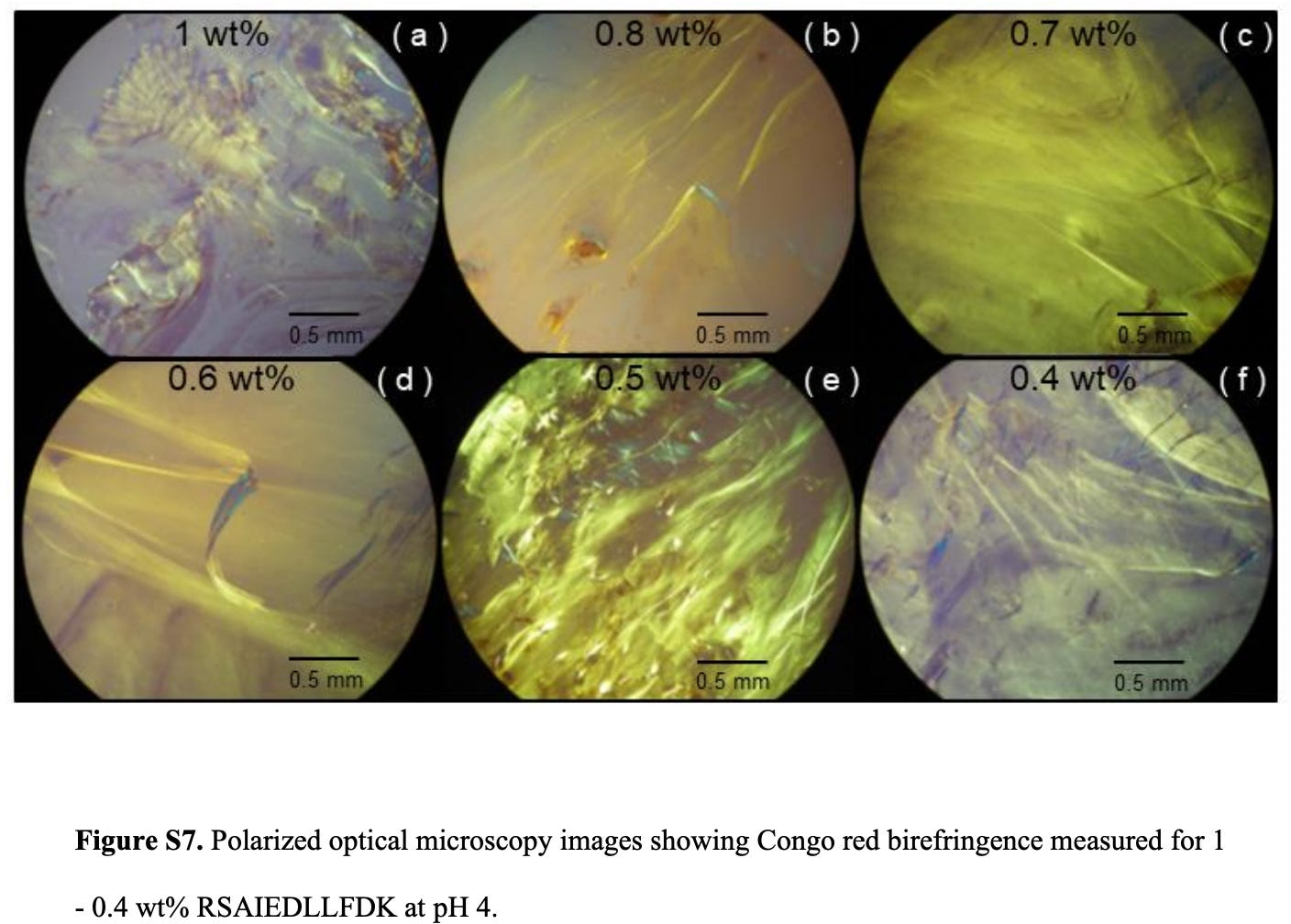
The above structure reminds me of the nanotapes that I wrote about studied here at 0.6 wt%. The scale here makes this nanotape about 0.1 mm across or 100000 nm. These structures are both about 0.1 mm across. Having said this, the size similarity has little to do with the reality of the final size of a nanotape. I believe that left to ‘grow’ under the appropriate conditions for formation (pH = 4-5), they would keep growing. I would also imagine that if the above image of the ‘shiny’ object was a nanotape structure, that we might see a lot more of them. I need to look into this more closely. I am not sure at this point what I am looking at (no one bloody does) and am hesitant to make any conclusions yet, but I thought this was interesting.
This next image is even better. And quite freaky, for lack of a better word. Looks like quartz. It looks even more like it doesn’t belong there.
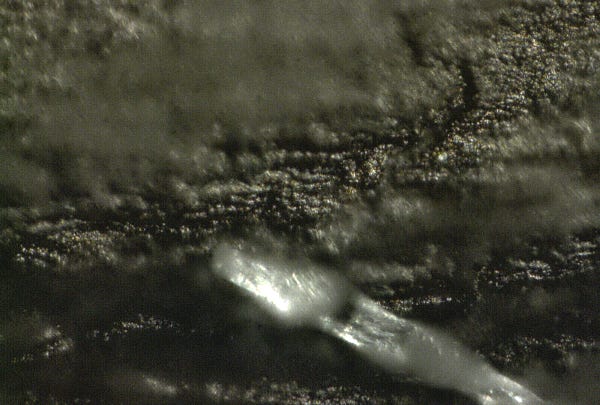
Crystal-like structures are attached to the bark-like structure of the ‘blood clot’ at 1000X magnification.
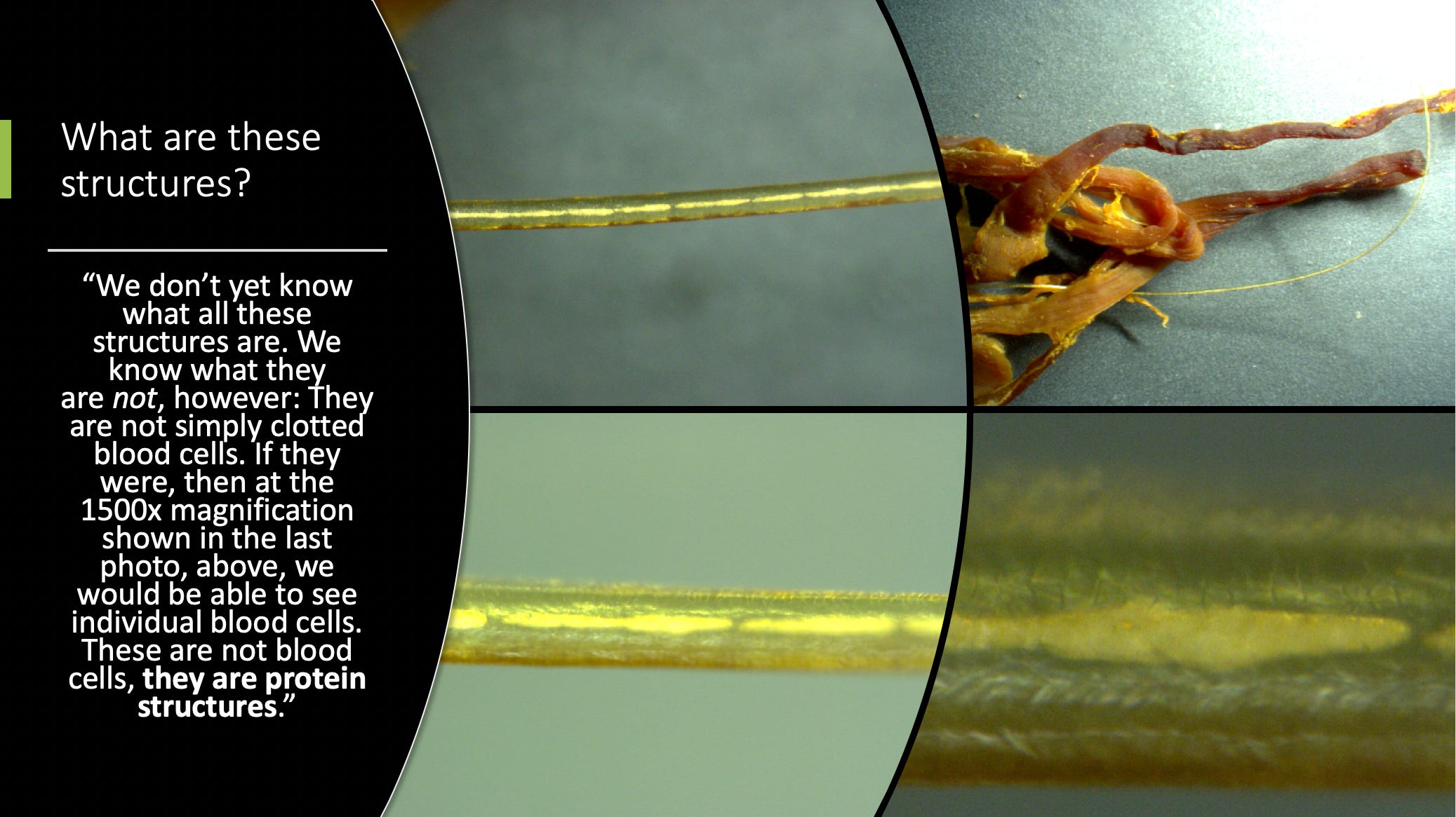
The person who did the analysis of these ‘clots’ said the following:
As you can see, these are in no way “normal” blood clots. These have structure and are fibrous. They are clearly being built by the body, using protein synthesis instructions to create this large mass that nearly resembles muscle tissue. Yet it is being built inside the blood vessels.
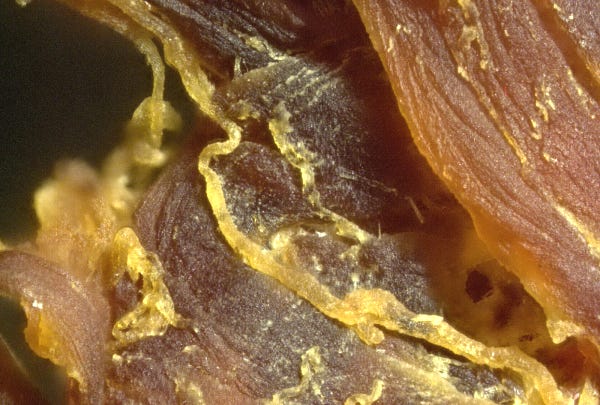
All of this is clot tissue that was found inside blood vessels or arteries at 100X magnification.
Finally, this fiber is not simply a human hair. It is firmly attached to the blood clot and when I tried to remove it, it would not tear away easily. This is not a contamination issue, it is a structure emanating from the clot itself.
The pathologist doesn’t know what these are. The embalmers don’t know what these are. But they know what they are not.
In conclusion, they are not “blood” clots. They are structures in the blood. They are “structural clots” or “fibrous clots” that are extremely large and are being constructed inside the body over time.
My grave concern is that every person who has been injected with mRNA instructions may be constructing these fibrous structures inside their bodies at this very minute, and that it’s only a matter of time before they block major arteries or cause heart attacks, strokes or other acute causes of “Sudden Adult Death Syndrome” (SADS).
I believe these structures may very well explain why so many seemingly healthy adults are suddenly dying.
Amyloidosis, amyloid or beta-amyloid plaque formation is known to be associated with the brain and neurons. But what if these spike-related amyloidogenic proteins didn’t have a neural preference?
Below is case of Cardiac amyloidosis from C. Michael Gibson, M.S., M.D. and Cafer Zorkun, M.D., PhD.

This is a higher-power photomicrograph of the heart tissue from this case. Note the amyloid deposition throughout the myocardium (1) as well as deposition in the wall of the blood vessel (2).
To quote some smart people:
“Follow a theory, spend loads of [money] trying find a drug and then, if it doesn’t work or produces serious side effects, dump the programme. What is needed is a much more holistic approach to the whole disease, rather than trying to compartmentalise it neatly within an ‘amyloid hypothesis,’ a ‘Tau hypothesis’ or anything else.”1
This is what severe atherosclerosis looks like, by the way. Not the same as our strange long strands.

I think we are dealing with a devilishly insipid hand-crafted (modified) RNA whose protein by-products (that appear to be multi-dimensional), following either translation, or digestion for MHC presentation, are amyloidogenic. Clinical presentation = systemic plaques/proteination of affected areas/tissues/vessels.
The location of the plaque formation/proteination would depend on many factors such as:
- whether or not the injection was intra-muscular or into the blood,
- the initial bio-distribution of the LNPs,
- the efficiency of delivery of the modified RNA payload,
- the integrity of the modified RNA template,
- the rate and efficacy of translation,
- the products of translation (which would depend on template(s),
- the immune response to the presence of the foreign proteins,
- the immune state of the individual prior to injection (chronic low level inflammation?)
just to name a few.
I think it is possible that the myocarditis cases being reported are due to Cardiac Amyloidosis. The primary symptoms of Cardiac Amyloidosis are shortness of breath, fatigue, swelling in the legs, heart palpitations, lightheadedness – pretty much the same as myocarditis (breathing difficulties, chest pain, fatigue, swelling in the legs, rapid heartbeat, lightheadedness and flu-like symptoms).2 3 These lists are pretty identical and I got them from 2 different sources.
I leave it here for now. A bit sensational, isn’t it? 🙂
I want to add Ryan Cole and Steve Kirsch’s interview here. Ryan is a pathologist and explains a lot of this here very well. Here’s a screenshot of one of the fibrous stringy things he pulled out of someone that he holds up at the end of the interview next to the one from this article.




0 Comments