


Why Do Vaccines Fail to Prevent Disease Transmission?
by A Midwestern Doctor | Oct 26, 2022
Many of you have been treated in horrific ways by your friends and family throughout the pandemic for refusing to adopt the nonsensical or dangerous pandemic management strategies that were force-fed to us by the media.
A key point I have tried to lay out here was that these strategies were known to be nonsensical from the start (they were designed to create compliance not to prevent deaths) and many approaches that would have been highly effective to save lives or prevent the economic devastation of COVID-19 were deliberately not implemented.
Note: Many broad claims are made here. Throughout this article, sources are provided for articles that provide the evidence to substantiate these claims.
The most plausible explanation for this inexcusable behavior was that oligarchs like Bill Gates chose to copy the playbook Fauci used throughout the early days of AIDS. At that time, highly effective treatments for AIDS were kept away from the public so that highly lucrative and extremely dangerous drugs could instead be forced upon a desperate population, resulting in many homosexual men being sacrificed to enrich a small number of predatory oligarchs.
In the case of COVID-19, remdesivir, a dangerous and ineffective (but highly lucrative) medication initially occupied that niche. Aided by the relentless efforts of corrupt members of the federal government, remdesivir was given a monopoly over hospital care for COVID-19 patients. Through its abysmal failure to cure the disease, remdesivir set the stage for “emergency” vaccines to enter the market, an “emergency” that only existed because effective treatments were kept out of the hospital system thanks to remdesivir’s monopoly.
Due to the emergency nature of COVID-19, many necessary vaccine development steps were skipped, and a few extremely questionable vaccines were allowed to enter the market. Because individuals, such as Bill Gates, who invested large amounts of money in the COVID-19 vaccines, also held significant financial influence over the media and tech platforms, none of these red flags were ever brought to the public’s attention, and the vaccines were instead hailed as the second coming of our lord and savior.
Once it became clear the vaccines were both unsafe and ineffective, all of the institutions that promoted the vaccines instead chose to aggressively censor any suggestion the vaccines could be harmful and engaged in a variety of highly manipulative tactics to force the public into taking as many vaccines as possible. As a result, an incalculable degree of damage has occurred and I suspect that we have still only seen the tip of that iceberg.
For science to function, an open debate is required. Unfortunately, in recent years (I believe this change was initiated during Obama’s presidency) support of the scientific process has been replaced with blind faith in things claiming to be “science” even though they do not follow the scientific process. Since that process was not followed throughout the pandemic, many atrocious policy decisions were allowed that resulted in disastrous outcomes for millions. This has created a widespread mistrust of countless institutions that have remained mostly unchallenged for decades, and it is my sincere hope the political will now exists for a once-in-a-lifetime opportunity to reform some of them.
There were many serious potential issues with the COVID-19 vaccines which were identified long before the vaccines came to market, yet due to the climate of corruption within the government, routine stifling of scientific debate, and mass censorship, none of these concerns were addressed before the vaccines entered the market.
I and many others lacked the immunological expertise and access to proprietary “data” scientists within the major vaccine manufacturers had. Despite this, each of us was able to independently predict exactly what issues would emerge with the vaccinations. Because of this, I must assume that the issues were also known ahead of time by the vaccine manufacturers.
For example, from the start, it was apparent that the vaccines would be ineffective in preventing COVID-19 (there was a lot of ignored evidence suggesting this was the case) and it was suspected the vaccines would cause the virus to rapidly mutate into variants the vaccines did not cover, thereby destroying what little efficacy the vaccines did have. Before we go further, I would like to request that you review this remarkable two-minute video, especially in light of the fact it was made over a year ago.
As you can see from the trend shown in this video, at any point during its progression, it was reasonable to consider that the vaccines might eventually reach a negative efficacy (meaning those who are vaccinated were more likely to get COVID-19 or die than the unvaccinated), which ended up being exactly what happened (e.g. this recent study is one of many datasets demonstrating that trend). Unfortunately, rather than reverse course, over the last year, those in charge chose to double down on vaccination and institute harsher and harsher vaccine mandates. This severely harmed millions of Americans (along with many more outside the United States) and gave birth to a policy of requiring an ever-increasing frequency of COVID-19 boosters to take the place of a permanently impaired immune system and rapidly waning immunity following vaccination.
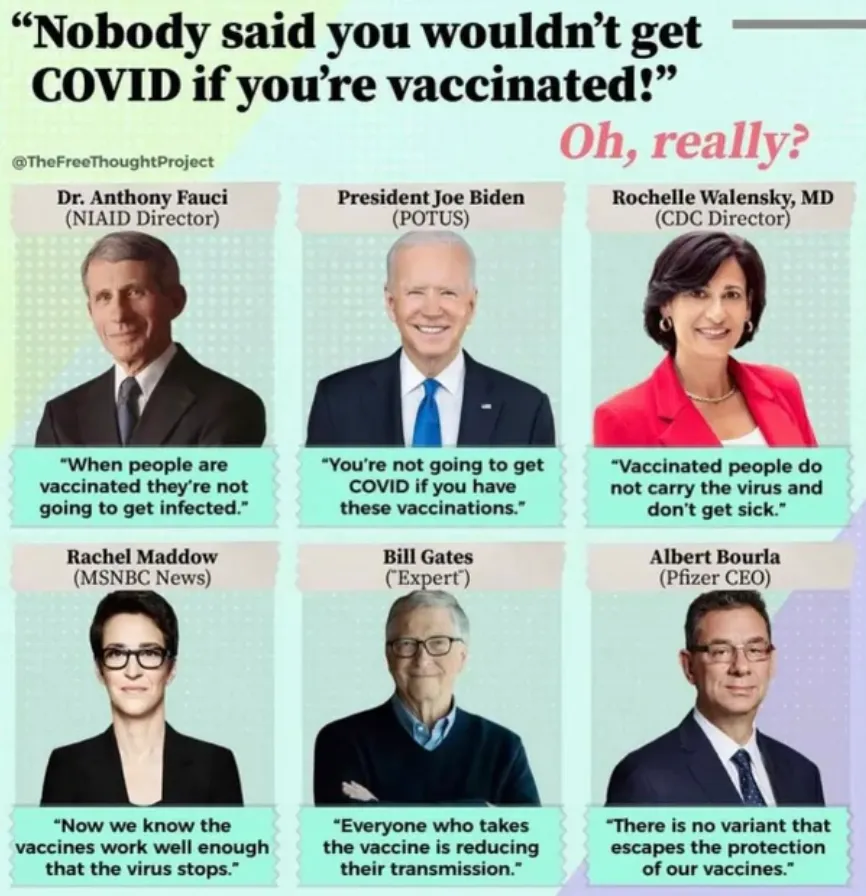
To overcome the widespread public resistance against these highly controversial vaccines, a variety of approaches that have previously been utilized to promote many other vaccines were implemented. One of the most critical ploys was to claim the vaccines reduced disease transmission and created herd immunity, thereby making your choice not to vaccinate both selfish and immoral since not vaccinating allegedly put the most vulnerable members of society at risk of dying. As I showed in the previous article, vaccine manufacturers, healthcare authorities, and the media all continually asserted this lie, yet are now attempting to gaslight us by claiming they were transparent from the start about their vaccines not preventing transmission.
When examining this behavior, the question becomes: was this misinformation due to (unfathomable) incompetence, or was it a result of deliberate lies? Although it is immensely difficult to read another’s mind (there is a rather high standard to prove intentional lying is occurring), I attempted to provide the clearest evidence I had to suggest our elected officials (and media agencies) were either lying or criminally negligent in stating the vaccines preventing transmission. Specifically, I quoted an October 2020 article that was written in a premier medical journal (and hence every public health official should have been familiar with):
Yet the current phase III trials are not actually set up to prove either (table 1). None of the trials currently under way are designed to detect a reduction in any serious outcome such as hospital admissions, use of intensive care, or deaths. Nor are the vaccines being studied to determine whether they can interrupt transmission of the virus.
Vinu then provided the best evidence I have seen showing our officials were intentionally lying to us. In May 2021 Fauci claimed vaccinated people become ‘dead ends’ for the coronavirus, while simultaneously publishing a prestigious May 2021 journal article stating the exact opposite (I largely agreed with this article). Given that this article demonstrates Fauci and his close confidants were completely aware of the science of vaccine prevention of transmission, it must be concluded that Fauci deliberately lied to the American people. I thus believe there is value in reviewing exactly what was known about vaccinations and disease transmission prior to COVID-19.
What is Herd Immunity?
As I was putting together this article, I realized that one of the major issues we face when evaluating this topic is determining exactly what constitutes “herd immunity” ( a surprisingly flexible term) and how to evaluate if a vaccine improves or worsens each rendition of it. Some of the criteria one may consider are as follows:
•Does the vaccine provide sterilizing or symptomatic immunity?
•Does the vaccine create asymptomatic spreaders?
•Does the vaccine promote more (or less) harmful variants?
•Does the vaccine cause the disease to infect different age groups?
•Does the vaccine increase or decrease disease outbreaks?
•Does the vaccine itself “shed” and infect others?
•Does the disease mutate faster than new vaccines for it can be developed?
•Does the vaccine improve or worsen the immune response to a pre-existing infection?
•Does the vaccine affect communal boosting of an infection?
•Does the vaccine improve or weaken the immune response to variants not covered by the vaccine and other related pathogens?
•Does the vaccine interfere with the production of protective maternal antibodies to the infection?
In this article, we will review how each of these has been influenced by other vaccinations in the past.
Herring’s Law of Cure
Modern medicine has a few foundational differences from nearly any other medical system that preceded it. One of the most important differences is that the modern medical approach seeks to dominate both human physiology and disease so that the intended medical outcome can be achieved instead of working in harmony with the natural physiology and healing capacities of the body to arrive at the desired outcome. In some ways, this is helpful (especially for emergencies), but it frequently falls short and results in more harm than benefit occurring from each forceful medical intervention that it utilized.
In order to maintain the modern medical paradigm, many of the natural physiologic, emotional, mental, and spiritual processes of the body must be ignored. One important but neglected process we must consider here pertains to routes of exposure.
Within homeopathy, there is a belief (Herring’s Law of Cure) that pathogenic factors enter the body superficially, and if they are allowed to penetrate deeper within the body, create serious or chronic complications. Curing chronic illness in turn is viewed as the process of encouraging disease to move from inside to outside the body. Chinese medicine holds a similar perspective and argues that the defensive energy of the body (Wei Qi) functions to prevent external pathogenic factors from penetrating into the body, and maps a progression of increasing severity of disease as the pathogenic factor travels from the superficial to the deep energy channels of the body.
I personally believe in this model and I have had many patients with disease histories that perfectly demonstrated this process. To some extent, I believe many of these observations can be attributed to a pathogenic factor inducing blood sludging, which initially occurs in smaller vessels (e.g. capillaries) and as the condition worsens, blood sludging occurs in larger blood vessels where its consequences are much more severe.
Historically, some of the earliest examples I know of for Herring’s Law of Cure came from observations of the effects of smallpox vaccination. There, it was observed by countless physicians that individuals who developed violent skin reactions to the smallpox vaccine typically suffered no significant complications from vaccination, whereas those who had minimal reactivity to the smallpox vaccine (suggesting the body was unable to mount a response to expel it) suffered a wide range of severe complications from vaccination unless a homeopathic (Thuja Occidentalis) was administered to expel it.
Sadly, this concept is not understood within Western medicine, and as a result, signs that the body is attempting to expel a pathogenic factor (e.g. a rash or a fever) are interpreted as the disease itself, and many therapies are thus aimed at suppressing these uncomfortable responses. This is particularly unfortunate as the onset of chronic illnesses often follows that suppression (e.g. autism onsetting in a febrile child after they are administered Tylenol).
To share a more contemporary example, there is some data to suggest that taking medications that reduce fevers (e.g. Tylenol or ibuprofen) worsens the severity of COVID-19 (sadly this has been the standard early treatment for COVID-19 throughout the pandemic). Similarly, I found that one of the more helpful remedies for COVID-19 (both for decreasing the discomfort one experiences and accelerating the resolution of the illness) is not to take a fever-reducing medication, but rather to heat up a febrile patient (especially if this can be done with infrared light). From both my own experiences and those of my patients, I now believe some of the discomfort one experiences during a fever is not from the heat of the fever itself but rather the internal strain the body is going through as it attempts to increase its temperature (which is eliminated if the body is externally heated).
Routes of Exposure
Many holistic systems including Chinese medicine and homeopathy argue that vaccinating through intramuscular injections is unwise because it allows a pathogenic factor to penetrate deep inside the body. This concern exists both for the reasons outlined in the previous section, and because the natural route of exposure the body relies upon to build immunity is bypassed when vaccines are directly injected. For example, this is how a foundational Chinese medicine textbook discusses this topic:

The issue with bypassing the natural routes of exposure is also acknowledged within immunology (and was referenced in Fauci’s May 2021 paper). Briefly, different types of antibodies are formed in response to an infection. One, mucosal IgA, is formed when a pathogen or components of a pathogen contacts the lining of your respiratory or digestive tract, and since this is the most common way pathogens enter your body, significant resources are devoted to producing mucosal IgA. Other types of antibodies (e.g. IgG and non-mucosal IgA) are instead produced when a pathogen or its antigenic components are present within the bloodstream.
A key thing to understand about this process is that infections often do not progress to the point they can overcome the mucosal IgA immunity, and thus never enter the bloodstream, while at the same time, immunity developing within the bloodstream does not trigger the development of mucosal IgA immunity. This is extremely important because most vaccinations are injected directly into the bloodstream and thus cannot trigger the production of the antibodies that normally allow us to resist becoming infected.
A recent paper explains in much more detail why the COVID-19 vaccines fail to produce mucosal immunity. Unfortunately, although this issue was recognized in immunology at least 30 years ago, most of the vaccines on the market are injected directly into the body and do not produce mucosal immunity. At this point, I believe our steadfast adherence to injectable vaccinations is a product of both our societal faith in the entire ritual of vaccination (which does not occur following non-injectable vaccinations) and the additional difficulties that arise from vaccinations administered in other manners (e.g. a nasal spray).
Nasal Irrigation
One of the fascinating things I learned about COVID-19 early in the pandemic was that the virus spends a significant amount of time replicating within the nose, sinuses, and throat before it gradually travels down the respiratory tract, enters the lungs, and then enters the bloodstream (note: the time it spends doing so is lengthened for Omicron). For this reason, it is often possible to treat COVID-19 in the early stages of infection by rinsing out the nose, throat, and sinuses (often while simultaneously applying a disinfecting agent to those areas which can neutralize the virus).
A variety of studies have been performed showing this approach is remarkably effective at preventing and treating the early stages of COVID-19. In my own experience (I use a mixture of concentrated xylitol crystals and dilute hydrogen peroxide) this approach can often provide immediate and significant benefits for a COVID-19 infection. Given how simple, accessible, effective, evidence-based, and safe the nasal irrigation approaches are, I believe it is inexcusable that public health authorities never disclosed them to the public.
There is also some evidence to suspect that nasal irrigation decrease viral levels and transmission which makes sense as this is a key area respiratory viruses inhabit and are expelled from as you breathe (thereby facilitating transmission). Clinical trials have looked at this issue and the only completed study I know of found nasal iodine rinses over the course of a day decreased COVID-19’s viral load within the sinuses.
This entire subject is relevant to the topic of transmission because much of the story of COVID-19 occurs within the upper respiratory tract (nose, sinuses, throat, etc.). If it is not possible to prevent COVID-19 from infecting the upper airway by inducing the production of mucosal IgA, it is extremely naïve to assume the vaccine can do anything besides prevent the development of symptoms in infected individuals— prevention of infection or transmission of COVID-19 cannot be obtained from an intramuscular vaccination.
While it could be argued that the need for vaccines that produce mucosal antibodies was a hard lesson that was only learned from events of COVID-19, the reality is that this was well known long before COVID.
Strain Replacement
In many cases, vaccines do not work at all (e.g. for influenza). In cases where vaccines do work, they will often create an evolutionary pressure that creates the emergence of strains that are resistant to the vaccine (this is analogous to bacteria eventually developing resistance to antibiotics that are used on them). As a result, when successful, vaccination campaigns often create a brief decline of the disease that is then followed by the disease rebounding to its original levels, and often changing to become more dangerous or affect demographics the disease did not infect before (who are typically older than the original susceptible demographic).
This cycle of futile attempts at disease eradication has been repeatedly demonstrated, with the strongest evidence of strain replacement existing for Haemophilus influenzae, Streptococcus pneumoniae, and Bordetella pertussis (each of which many of our children are mandated to be vaccinated for). These bacteria are particularly susceptible because the vaccines against them only use a few specific proteins, which makes relatively few mutations be required for the bacteria to evade the vaccine.
Similarly, a major issue with the COVID-19 vaccines is that they only contain the spike protein (which was a rapidly mutating part of the virus to begin with). For this reason, it was virtually assured variants with spike proteins the vaccine did not protect against would emerge following vaccination campaigns that created a selective pressure for their emergence.
As far as I know, there are only two ways to prevent the strain replacement issue:
1. Utilize a vaccine that does not place selective pressure on the organism in question.
•The tetanus vaccine (which provides immunity to the tetanus bacteria’s toxoid rather than the bacteria itself) and the diphtheria vaccine (which does the same thing), are the best examples of this approach.
•For tetanus, this approach, at least in theory, makes sense. The bacteria lives everywhere and is not transmitted from person to person (rather it is transmitted by having tetanus inoculate a deep wound). The only sensible target for a vaccine is thus to prevent the bacteria’s toxoid from causing a fatal complication, and someone becoming immune to the toxin will not influence the bacterial population around us.
•For diphtheria, the organism essentially ceased to exist in the Western world, likely due to improved living conditions (and possibly antibiotic treatment of the disease) rather than vaccination. Since the infection is unheard of now in the first world, vaccination is unlikely to affect its evolution because it does not exist to begin with. Furthermore, like tetanus, the diphtheria vaccine targets the bacteria’s toxin (which is not necessary for the survival or replication of the bacteria) rather than the bacteria itself, so selective pressure to evade the vaccine does not exist. Decades of studies likewise have shown that the diphtheria vaccination has no influence on the likelihood one will carry or transmit it. Unfortunately, despite this infection now being non-existent, five vaccinations against it are still required for all children in America.
2. Utilize a live attenuated vaccine.
Note: with the exception of the tuberculosis vaccine, which is not required in the United States, all live attenuated vaccines are viruses.
•By containing the entire pathogen, there are enough antigens present to prevent the pathogen from evolving resistance to all of them at once. Because of this, it is highly unlikely a variant will emerge that effectively resists the vaccine (similarly, were this not the case, the immune system would have failed to protect us and doomed our species early in its evolution).
•The primary problem with this approach is that the organisms constituting the vaccine are still infectious and can shed to others. For this reason, immunosuppressed people are advised not to receive the vaccines, often advised to not be around recently vaccinated individuals, and periodic disease outbreaks can be traced to these vaccines.
Now that we have reviewed some of the common issues with vaccinations that consistently prevent herd immunity from emerging, we shall review how those lessons were repeatedly learned in the past with other vaccinations. Public health officials frequently attribute disease outbreaks to an insufficient percentage of the population being vaccinated to attain herd immunity, yet in almost all cases, that threshold is never met, or if it is met, it is raised again and again after it fails to produce its originally promised result. My hope is that the rest of this article will help you to understand why that is.
Note: Many of the studies contained in the following sections were sourced from Miller’s Critical Review of Vaccine Studies and Turtles All the Way Down.
Smallpox Vaccines
The subject that originally brought me to write here was the realization that our pandemic response was re-creating the smallpox catastrophe. Conventionally, it is believed that smallpox vaccinations were responsible for eliminating the scourge of smallpox, and this is such a foundational belief most never think to question it.
However, an alternative narrative also exists. In the pre-vaccine era of deadly infectious diseases, humans lived in abysmal living conditions that were highly destructive to the immune system and highly conducive for spreading numerous (often deadly) infectious diseases. Many progressive activists of the time in turn fought tooth and nail for over a century to improve the standards of living across the Western world so that the lower class would not be forced to live in absolute squalor. As best as I can tell these shifts were a result of an economic need to move the lower class into hastily assembled jam-packed cities to provide the workforce needed for the industrial revolution, although there is some evidence to suggest the living conditions were intended to mitigate population growth.
These activists were ultimately successful, living conditions improved and there was a stark decline in all infectious diseases. Much of the societal mythology behind the medical profession is predicated upon vaccines conquering the dark era of infectious disease, when in reality, it simply took credit for the tireless work of these early activists.
In the case of smallpox, as detailed in my first article, the smallpox vaccines would consistently fail to prevent smallpox and frequently severely injured those who received them, leading to growing working-class opposition to vaccination. The medical profession initially opposed the smallpox vaccine because they knew it was unproven, unsafe, and ineffective, but as doctors’ livelihoods revolved around administering it, they gradually warmed up to it, and in time, began covering up both its failures and severe injuries.
This dynamic was particularly problematic because smallpox vaccination campaigns would cause rather than prevent smallpox outbreaks. Due to the investment both governments and the medical profession had in the vaccination, these failures were interpreted as a result of insufficient vaccination rather than the vaccine itself being the problem. A positive feedback loop was hence created resulting in more and more draconian mandates being forced onto a non-compliant population as the vaccine failures mounted.
Eventually, one English city held a historic protest against vaccination attended by citizens across Europe, resulting in a government being installed that chose to manage smallpox by improving public sanitation, quarantining sick patients plus their contacts, and making vaccination optional. Vaccination rates plummeted, and the medical profession predicted an apocalyptic smallpox outbreak in this city, but instead, its approach proved successful, and once it was copied by the rest of the world, resulted in the elimination of smallpox.
If a vaccination causes outbreaks, it is reasonable to assume it will be unlikely to create “herd immunity.”
Influenza Vaccines
Before entering medicine, I noticed I would periodically come across people whose health had permanently gone downhill after an influenza vaccine. Once I entered the medical field, I noticed that every year the manufacturers would incorrectly model which strain would be dominant during the current influenza season.
Because the incorrect strain was chosen for that year’s vaccines, year after year, my colleagues would lament that this year was going to be a “bad” flu season. Despite recognizing the vaccine had essentially failed, they would simultaneously argue that the influenza season would have been much worse had there not been a vaccine, and therefore that it was critical for everyone to get vaccinated (which may be where the current meme of individuals afflicted [often severely] with COVID-19 being grateful they were vaccinated originated from).
Keeping all of this in mind, I made a point to locate the vaccination history of influenza patients I encountered in the ICU and noticed that each patient I could legally access the records of had been vaccinated that year and often the year before. As a result, I was not the biggest fan of this vaccination and had strong objections to it being mandated on healthcare workers.
Original Antigenic Sin represents one of the best explanations I have encountered for this phenomenon. OAS posits that vaccination reduces the body’s ability to mount an immune response to viruses not matching the vaccine (e.g. other variants of the same species or other species entirely). In my opinion, OAS has been best demonstrated with the influenza vaccine, and to quote the Lancet:
However, there is a potential downside to yearly seasonal influenza vaccination that has not been given much thought. In theory, effective vaccination of children against seasonal influenza A viruses might prevent the induction of heterosubtypic immunity otherwise induced after productive, in most cases, self-limiting infection of the upper respiratory tract. This interference with the induction of heterosubtypic immunity might not be important under normal circumstances, but in context of the pandemic threat caused by HPAI A H5N1 and the pandemic outbreak of new influenza A H1N1 viruses, the presence or absence of heterosubtypic immunity might affect the clinical outcome of infection with the new pandemic strain. Consequently, we hypothesised that effective vaccination against seasonal influenza interferes with the development of protective immunity against a lethal infection with an influenza virus of a new subtype (eg, H5N1).
Many studies in turn have suggested routine influenza vaccination increases susceptibility to the more dangerous strains of the virus:
A review of four studies found that recipients of a seasonal influenza vaccine had a significantly increased risk (ranging from a 40% to 150% increase) of subsequently developing severe pandemic influenza (which unlike normal influenza could hospitalize you).
A 2010 study of the severe pandemic influenza found that active duty members of the military were more likely to have received influenza vaccination than were those without H1N1 virus infection. The authors of this paper did not believe this represented a true association but did not provide the data to independently verify that assessment.
A 2009 study found that vaccinating mice for influenza removed their ability to develop resistance to pandemic influenza following previous exposure to normal influenza (whereas this paper demonstrates that prior influenza exposure without an influenza vaccine typically creates immunity). Compared to unvaccinated mice, vaccinated mice continued to lose body weight after a pandemic influenza infection and had 100-fold higher lung virus titers on day 7 [this increases transmission] post-infection and more severe histopathological changes.
This 2013 study found receiving an influenza vaccination two years in a row increased rather than decreased the likelihood of developing influenza.

A 2013 Cochrane review (note: this was written shortly before this group which had previously been the gold standard for appraising scientific evidence was bought by Gates and stopped producing quality work that challenged vested medical interests) found:
We could find no convincing evidence that [giving children] vaccines [for influenza] can reduce mortality, hospital admissions, serious complications or community transmission of influenza…Despite the great variety of method variations, the reviews [of vaccinating various groups for influenza] all have similar conclusions to those of our 2005 Cochrane Review: trivalent inactivated vaccination has few effects and there is no evidence that it affects deaths, complications or transmission of influenza. Live attenuated vaccination performed a little better at the expense of safety.
This 2016 Cochrane review specifically assessed the effect of vaccinating healthcare workers and found it had no effect in reducing influenza cases in their facilities or hospitalizations. This 2012 article also highlighted that there was no scientific evidence that influenza vaccination of healthcare workers protected patients and that it was unethical healthcare workers were being mandated to vaccinate.
This 2012 study conducted between 1999-2007 of 261 children 6 months to 18 years old who developed laboratory-confirmed influenza found that infected children were 267% more likely to be hospitalized if they had previously received an influenza vaccine.
A 2012 study randomized 69 children to receive an inactive influenza vaccination, and 46 to receive a placebo. Of those vaccinated, 29.0% developed an infection with a non-influenza upper respiratory virus, whereas 3.4% of those who were not vaccinated developed an upper respiratory infection from a non-influenza virus.
This 2006 study (similar results can be found in other data sources) showed that when 18 years of data were reviewed, the influenza vaccine has little or no effectiveness over the U.S. population for preventing influenza cases, hospital admissions, or deaths. It also highlighted that a significant risk of influenza disease transmission exists with live attenuated influenza vaccinations.
A 2009 review from the British Medical Journal of 259 studies on Influenza vaccination attempted to summarize the current scientific literature and found:
Most of our studies (70%) were of poor quality with overoptimistic conclusions — that is, not supported by the data presented. Those sponsored by industry had greater visibility as they were more likely to be published by high impact factor journals and were likely to be given higher prominence by the international scientific and lay media, despite their apparent equivalent methodological quality and size compared with studies with other funders.”
A 2013 article from JAMA by Peter Doshi (who later correctly identified numerous red flags in the COVID vaccine trials), presented strong evidence that health authorities consistently exaggerate the dangers of influenza and inflate the benefits of influenza vaccination. In a separate 2013 BMJ article, Doshi showed that marketing strategies by authorities designed to increase influenza vaccinations (which before COVID-19 were the most widely visible public health initiative in the Western world) lack moral integrity and scientific support.
A key point Doshi mentions is that the majority of upper respiratory illnesses are caused by viruses other than influenza, thereby making claims influenza vaccines can prevent them disingenuous and also helping to explain why cases of influenza “disappeared” once the pandemic incentivized providers to instead classify all those other illnesses as COVID-19.
From reading the evidence provided within this section, many parallels to the COVID-19 vaccination campaign should be apparent as many of the exact same issues have again emerged (e.g. negative vaccine efficacy). Unfortunately, despite often being ineffective and unsafe, healthcare authorities for decades have trumpeted the absolute necessity of these vaccines, and everyone within the medical field has been forced against their consent to take them under the flawed argument that they will protect one from illness and from transmitting the disease to those around them.
It is my personal belief that if this injustice had been addressed prior to COVID-19, it would not have been possible to force mandatory vaccinations upon the population. By being made first in line for vaccination, healthcare workers were used to initially market the vaccines and their longstanding influenza vaccine mandates were used to argue that a precedent already existed for vaccine mandates being justified once the general population complained about the mandates.
Overall, I believe influenza vaccinations have the greatest overlap with the COVID-19 vaccines (e.g. consider that like the influenza advocates, the COVID-19 vaccine proponents are all pivoting to continual boosters for each new variant). As the evidence in this section demonstrates, it is highly unlikely a vaccination for a rapidly mutating respiratory RNA virus can ever produce “herd immunity.”
Finally, although influenza vaccines have been touted as a critical measure for the prevention of COVID-19 there is now some evidence to suggest that influenza vaccines increase rather than decrease one’s risk for a severe COVID-19 infection. In addition to the recently uncovered evidence, prior to COVID-19, one study had shown that influenza vaccinations increased one’s risk of a coronavirus infection by 36%.
Diphtheria Pertussis Tetanus Vaccines
DPT is a remarkably dangerous vaccine and is likely a primary cause of sudden infant death syndrome. Because of the toxicity of the original pertussis vaccine, a less dangerous (acellular) formulation of it was adopted that was less effective at providing sterilizing immunity as it lacked many of the antigens found in the whole cell formulation.
Presently, the DPT vaccine contains three toxins (those produced by diphtheria, pertussis, and tetanus) along with certain proteins pertussis uses to attach to the respiratory tract (varying combinations of filamentous hemagglutinin, pertactin, and fimbriae types 2 or 3). There are two key issues with this approach:
•By promoting resistance to a few key proteins pertussis needs for survival, this promotes the evolution of variants with different proteins (e.g. vaccination has made pertactin much rarer in circulating pertussis strains, and one colleague who is a specialist in this area believes it is no longer present in strains within the United States).
•By creating immunity to the pertussis toxin (which is what causes whooping cough) but not the bacteria itself, vaccination increases the likelihood of developing asymptomatic pertussis infections.
One of the most conclusive studies on this phenomenon was performed in 2014. In it, baby baboons (which have one of the most similar responses to pertussis as humans) were subjected to 4 conditions: no exposure to pertussis, exposure to pertussis leading to natural immunity, or vaccination (at 2, 4, and 6 months of age) with either the acellular or whole cell vaccine. Following completion of their initial protocol (e.g. one month after the third vaccination) they were exposed to pertussis, and then later placed with other baboons. From this, it was found that:
•Baboons with natural immunity to pertussis did not become colonized by pertussis, did not develop symptoms, and due to this lack of colonization, likely did not transmit pertussis to other baboons.
•Baboons with no prior immunity to pertussis developed symptoms, were infected with the bacteria for 30 days, and in a study prior to the 2014 one, were shown to transmit pertussis to other baboons without immunity to pertussis.
•Baboons that received the whole cell DPT vaccine did not develop symptoms and were infected with the bacteria for 18 days (transmission was not tested but was likely to have occurred due to their colonization).
•Baboons that received the acellular DPT vaccine did not develop symptoms, were proven to transmit pertussis and remained infected with the bacteria for 35 days.
This study (excluding another assessment of transmission) was later reconfirmed by the same research team and soon after similar results were found in mice by a separate team. Decades of studies in the real world have likewise shown pertussis outbreaks occur in vaccinated communities and that the acellular pertussis vaccines produce asymptomatic spreaders (this study estimated acellular pertussis vaccination campaigns increased the presence of asymptomatic spreaders by 30 times).
Additionally, like other vaccines (e.g. COVID-19), DPT suffers from waning immunity. A 2013 study evaluated waning immunity in 224,378 children in Minnesota children and 179,011 in Oregon who had received five doses of DPT (the 5th dose is given at 4-6 years of age). The likelihood of a symptomatic pertussis infection increased by 1.9 times 2 years after vaccination and 8.9 times 6 years after vaccination for those in Minnesota, and 1.3 times to 4.0 times for those in Oregon.
All of these results illustrate why herd immunity to pertussis cannot be achieved through the current vaccination approach. This has not stopped the pharmaceutical industry from aggressively marketing the vaccine (e.g. one campaign claimed unvaccinated grandparents pose a lethal risk to their grandchildren), and numerous unvaccinated friends of mine, at the urging of the child’s parent’s doctors have been banned from visiting their grandchild. Fortunately, that campaign was egregious enough for a lawsuit to be filed against the manufacturer on the basis of its commercial claiming the vaccine prevented transmission constituting false advertising!
Polio Vaccines
Two vaccines form the foundation of the mythology of Western medicine, smallpox which was discussed above, and polio. Like smallpox, when one pries into its story, a variety of issues with the conventional narrative emerge. From having looked through the subject in depth, the best explanation I have at this point for what occurred is as follows:
1. Widely used dangerous pesticides, (first lead arsenate and then later DDT) created neurological damage which mirrored the symptoms of polio (including pathologic changes directly observed within the spinal cord).
2. As this issue grew, public health authorities addressed it by sensationalizing the dangers of the polio virus (which, while not as pathologic as DDT, was also a problem and was worsened by various environmental cofactors) and creating a vague disease criteria that allowed many conditions not caused by polio to be diagnosed as polio.
3. Following the creation of this fear, a nationwide campaign was conducted to search for a polio vaccine and then vaccinate the country.
4. In parallel to the vaccine being released, DDT was withdrawn from the market, and the criteria for what constitution polio was made much more strict, so many things previously defined as polio no longer were considered to be polio.
All of this in conjunction created the perception that vaccines had performed a modern-day miracle and eliminated polio (despite the decrease in polio preceding the vaccine and much of the population which also experienced a decline having never been vaccinated). Because of this, a variety of diseases exist now (e.g. “Non-Polio Acute Flaccid Paralysis”) that previously would have been labeled as polio, but are now instead categorized differently. As far as I know, the misleading diagnostic reclassifications of polio and influenza are the closest parallels that exist to the hospitalizations and deaths that were erroneously attributed to COVID-19. Likewise, I expect when the government finally wants to end the pandemic, it will do so by tightening the criteria that must be met for an illness to be diagnosed as COVID-19.
In the case of polio, I believe one of the biggest factors that created the perception the medical field had triumphed over the scourge of polio was its switching from the widespread use of external negative pressure ventilators (iron lungs) to internal positive pressure ventilators (the standard ventilator). Positive pressure ventilators are much cheaper and easier to use (although negative pressure ones are much healthier for patients that require long-term ventilation), so once the technology was available the switch was made.
From a herd immunity standpoint, there are a few important takeaways from the polio story:
•Two vaccines were developed for polio. One was an inactivated injectable vaccination (the Salk vaccine) which was designed to provide immunity that prevented damage to the central nervous system from polio. Since this vaccine did not provide immunity to a polio infection, it could not prevent polio transmission. The other (the Sabin vaccine) was a live attenuated version of the virus that was administered orally and colonized the GI tract, providing mucosal immunity to polio, which at least in theory prevents transmission.
•The live vaccine periodically caused polio in its recipients (I know someone this happened to). For this reason, the inactivated polio vaccine is used in the United States.
•Although only the live vaccine is capable of producing immunity that prevents polio transmission, it is also frequently responsible for creating disease outbreaks from vaccine recipients shedding live attenuated vaccine viruses.
•Presently, the majority of cases of polio-like paralysis around the world (including high-profile ones that are used to argue for more vaccination) result from live polio vaccine shedding rather than the polio virus itself. In one of the most tragic cases where Gates diverted India’s public health budget to initiate a mass live polio vaccination campaign of India’s children there (often giving each child as many as 50 doses of the vaccine), it was estimated that his program caused 491,000 children to become paralyzed with a “polio-like” illness.
All of this again argues against it being possible to create herd immunity through vaccination, in spite of many public health figures lamenting otherwise.
Human Papilloma Virus Vaccines
Prior to COVID-19, the HPV vaccine was the most dangerous vaccine on the market. At the time that Gardasil was approved, its manufacturer Merck had just settled a massive lawsuit that required Merck to pay out 4.85 billion to patients who suffered heart attacks and strokes from Vioxx, an unnecessary drug they willfully concealed the side effects of (later in 2011, Merck had to pay another billion for their fraudulent marketing).
Sadly Merck’s negligent conduct with Vioxx left the company in a pinch where they needed a miracle drug to recoup their losses and Gardasil filled this role (leading many to nickname the HPV vaccine ‘Help Pay for Vioxx’). There had been longstanding hope in the industry that a “vaccine for cancer” could be made as the societal fear around cancer would make it an instant blockbuster, and it just so happened a viable product had emerged right when Merck needed one.
To produce a market for the vaccine, a hysterical marketing campaign took off to scare everyone as much as possible about cervical cancer. Thanks to pap smears, which were universally recommended in 1976, this somewhat rare cancer had already been in decline, going from 13.07 cases each year per 100,000 women in 1973–1975 to 6.01 per 100,000 women in 2006–2007 (for context each year breast cancer afflicts 128.3 per 100,000 women). A variety of factors are linked to cervical cancer (e.g. smoking doubles one’s risk) and Merck was able to position HPV as the sole cause of cervical cancer, leading to many changes in medicine that shifted cervical cancer prevention towards primarily monitoring for HPV. Merck in short sold the following sales pitch to the public:
•Cervical cancer is an urgent epidemic to address.
•The primary cause of cervical cancer is HPV.
•HPV can be effectively prevented with vaccination if you are vaccinated before you get infected and vaccination must thus precede any form of sexual activity.
•Every institution is hence obligated to push the vaccine on our children and to cover up any incidents of harm from the vaccine as this is a necessary price to pay for obtaining herd immunity from cervical cancer.
Sixteen years later, although we did as Merck insisted, cervical cancer has not gone away and arguably has increased (depending on the data set you look at). There is also a large body count from this vaccine, which per its own trial data is far more likely to harm than benefit each recipient, and I have numerous close friends and patients (who never would have gotten cervical cancer to begin with) whose lives were permanently altered by the significant complications they received from the vaccine.
With that background, let’s now look at some of the faulty assumptions behind the HPV vaccine.
In medicine, it is often very difficult to test the long-term effects of a drug, so instead of assessing those effects, “surrogate markers” which are believed to correlate with a positive effect are tested and it is assumed that if the surrogate markers improve in the short term, a significant benefit will arise in the long term. Sadly, however, this is often wishful thinking as the expected benefit does not materialize, and sadder still most regulators will accept improved surrogate markers as an indication a drug works. In the case of the HPV vaccine two surrogate markers I believe to have been erroneous were accepted by the regulators:
•Reducing HPV infections and precancerous inflammatory cell changes served as surrogate markers for the prognosis of developing cervical cancer (when in reality cervical cancer is multifactorial and requires numerous approaches to be addressed).
•Generating antibodies to HPV (which is what the vaccine was designed to do) was equated to immunity to HPV. Because these antibodies were difficult to generate, a very strong adjuvant was required to attain an acceptable antibody response (and likely accounted for the high rates of debilitating autoimmune complications from the vaccine). Interestingly, the CDC now acknowledges they do not know what degree of an antibody response is necessary to create immunity to HPV.
Additionally, Merck’s original trial data showed that if someone was infected with a vaccine strain (e.g. HPV-16) at the time of vaccination, the vaccine would instead increase their risk of developing cervical cancer (a -44.6% vaccine efficacy was observed), which is likely a consequence of inflammation being triggered at the site of a preexisting infection (inflammation in the cervix causes cervical cancer and this is likely why HPV, like smoke exposure, creates cervical cancer in the first place).
Although various petitions were sent to the FDA to require screening for HPV prior to vaccination, they and other medical authorities like the American College of Obstetricians and Gynecologists eventually decided it was unnecessary and everyone should be vaccinated regardless of previous HPV infection status (even though the need for early vaccination is marketed based on there being no cure for HPV and needing to be vaccinated prior to being exposed to HPV). I will also note that I have seen a rapid worsening of a preexisting HPV infection following HPV vaccination and I know two people who were vaccinated prior to becoming sexually active that had their pap smears turn positive for HPV shortly after vaccination.
I mention all of this because a somewhat common side effect of the COVID-19 vaccines is rapidly developing a severe or fatal COVID-19 infection. Many individuals have reported this to me, it has been reported in surveys I have reviewed, and it is a common cause of death in VAERS. I have also come across cases where the individual reported having a positive COVID-19 test, having minimal symptoms, and then immediately becoming severely ill with COVID-19 after vaccination.
Somewhat in parallel, although the vaccine was initially marketed as a treatment for long-haul COVID-19, I have come across numerous individuals who did just that and had their long-haul COVID-19 become much worse following vaccination. All of this has led me to suspect the COVID-19 vaccines modify the inflammatory response to COVID-19 in a detrimental manner (much of the harm of COVID-19 comes from the inflammatory response it elicits). However, like Gardasil, a pre-existing infection is never considered in the context of vaccination.
Note: Recently I completed an article covering the systemic corruption in the CDC which causes them to regularly push through dangerous vaccines. The CDC director who pushed through Merck’s Gardasil retired not long after it was approved and took a lucrative position as president of Merck’s vaccine division.
Chickenpox Vaccines
Note: This topic was discussed more extensively in this article.
Chickenpox is a relatively benign childhood illness that can become quite problematic if it recurs later in life as shingles. When the chickenpox vaccine (a live attenuated virus) was introduced, skepticism existed in the medical community towards it being needed. After it was brought to the market, an unexpected side effect emerged from the vaccine: a significantly increased incidence of shingles in the adult population.
It was eventually discovered this reemergence arose from the vaccine-reducing childhood cases of chickenpox in the community, which in turn caused adults in the community to no longer be regularly exposed to small doses of chickenpox. This loss of periodic boosting gradually weakened their immune response to the virus (this is a natural form of the waning immunity often observed after vaccination) and thus greatly increased the likelihood of them developing shingles.
The story of this vaccine is useful to consider as a potential consequence of developing an effective vaccine for a virus the human species had previously evolved a natural equilibrium with. This is particularly consequential with chickenpox as other vaccines (particularly those for COVID-19) are immunosuppressive and further increase the likelihood of developing shingles.
Measles
At the time the measles vaccine was developed, it was highly questionable if it was needed, or as the below graph shows, if it was responsible for the benefits attributed to it.

Because the measles vaccine was a live attenuated vaccine, it was effective at preventing one from catching the virus and did not trigger strain replacement. Unfortunately, altering the natural equilibrium with the measles virus removed the population’s ability to have true herd immunity to the disease, and instead required almost everyone to be vaccinated to prevent an outbreak from happening (further complicated by waning efficacy from the vaccine as demonstrated here in figure 3).
Prior to the era of measles vaccination, mothers would pass on immunity to their immunologically naive children through maternal antibodies, repeated boosting occurred through small exposures to the measles virus in the community, and a non-vaccine herd immunity had emerged. Since the measles vaccine campaign, this natural immunity has been lost and vaccination of most of the population until the end of time is now needed to prevent further outbreaks of measles (in other words we traded natural immunity for a perpetual sales product).
The most extreme examples of how measles interacts with populations lacking immunological exposure to it were observed in the Native American populations after measles was introduced by the Europeans and was one of the new infectious diseases recognized to devastate their populations. In one famous outbreak, 10% of those infected died. Given that no one died after the recent measles outbreak that was used to push through mandatory vaccination laws for children across America, we are clearly not facing anywhere as dire of a situation as the Native Americans, but examples like that illustrate why removing herd immunity has so many pitfalls.
Additionally, vitamin A supplementation dramatically improves the immune response to measles and many deaths from measles in the third world could like be prevented by pursuing a vitamin A supplementation approach. Unfortunately, due to the fanaticism with vaccination, this cheap and highly effective approach is rarely, if ever considered.
Note: there are other additional efficacy issues with the MMR vaccine. For example in 2010, scientists working for Merck (its manufacturer) filed a lawsuit against the company alleging Merck had fraudulently altered its antibody test results to claim the mumps portion of MMR was significantly more effective, which Merck needed to do so that they retained an exclusive monopoly on selling the vaccine within the USA. Somewhat supporting these allegations, in 2018, a Mumps outbreak occurred on a naval vessel in which all 703 crew members aboard had been vaccinated with MMR.
Alternative Approaches for Achieving Herd Immunity
Given that our synthetic attempts to achieve herd immunity have been less than successful, it is worth considering what alternative options exist. The first one pioneered by the Amish (who became the first group in the United States to achieve herd immunity to COVID-19) was as follows:
It should be noted that there were risks with this approach and a wave of deaths that impacted the Amish (and Mennonite) community at the start of the pandemic. However, the deaths were no different from areas that instituted much harsher lockdown policies, and before long as the above video shows, the Amish were able to return to their normal lives unlike many who have been stuck in the pandemic fiasco for the last few years.
The Amish approach was also utilized throughout Africa, which has fared much better throughout the pandemic than most of the far wealthier countries, especially as variants that evade vaccinations emerge (e.g. consider this comparison between an under-vaccinated and over-vaccinated nation). I likewise checked the most recent dataset I could find and found COVID-19 deaths in every African nation had flattened while deaths in nations with robust public health apparatuses have continued to climb. However, many of the news reports I have found discussing herd immunity in Africa state that Africa’s low vaccine uptake has made achieving herd immunity in these nations “impossible.”
The less extreme version of the Amish approach was outlined in the Great Barrington Declaration, which advocated for only isolating vulnerable members of society while working to develop herd immunity in the less vulnerable members of society (and in tandem strengthen their immune systems).
Scott Atlas, a critically thinking member of the COVID-19 task force astutely noticed any approach besides that outlined in the Great Barrington declaration would lead to more deaths and have massive economic and societal costs. Fauci and Birx in contrast adamantly opposed it and demanded perpetual lockdowns, masking, and mass testing throughout Trump’s presidency.
Periodically, Atlas would convince the task force to follow his approach, and in each case where he did, before the new guidelines became established, a leak would be made to the media. A hysteria would then break out across the airwaves stating Atlas and others wanted to sacrifice countless Americans for the greater good of achieving herd immunity forcing them to back off from this advice. Because of this, a policy like the Great Barrington declaration could never be enacted and we instead followed the disastrous approach Fauci and Birx advocated for which set the stage for the even more disastrous COVID-19 vaccine campaign.
In each generation, countless individuals in the natural medicine field have also looked at this problem. Each time, they have concluded the best solution to addressing devastating infectious diseases is some combination of effective (and often early) treatments for the disease, isolation of sick individuals, improving public hygiene, and additional supplemental measures needed to improve the immune system.
Unfortunately, time and time again, this approach is suppressed and ignored to enshrine the mythology of vaccination being the only possible way to approach the problem. Although many effective treatments were discovered for COVID-19 in early 2020 that could have ended the pandemic (I was heavily involved in one of the teams working to bring a viable treatment to the public and corresponded with many other researchers doing the same thing), each approach was widely disparaged, and to varying extents outlawed.
This greatly upset many of my colleagues who were in disbelief this could happen in America. Time and time again I counseled them to remember that this has always been how things go and that we were incredibly fortunate because unlike those before us, there was so much public support behind treatments not endorsed by the medical authorities that we had a once in a lifetime chance to change this paradigm no one before us had ever had access too.
Conclusion:
As all of the above examples illustrate, a variety of issues exist with widespread vaccination against an infectious disease. Most of these issues, despite being “unexpectedly discovered” with COVID-19 have been known about for decades, and have been allowed to perpetuate because the public health field has been allowed to claim whatever they want (which is always the absolute necessity of more vaccines) without external accountability for those claims.
Given the frequent futility of vaccination and the routine suppression of effective alternatives, this then raises the question as to what motivates their aggressive promotion onto the marketplace.
The simplest answer is that the primary reason for their promotion is the love of money. If a company (or a federal vaccine regulator) can produce a vaccine that is added to the vaccination schedule, the guaranteed market created by doing generates a financial windfall. To further sweeten the deal, unlike most pharmaceutical products, no liability can be incurred by a vaccine manufacturer (which is an irresistible incentive in the pharmaceutical business).
For this reason, unnecessary and unproven vaccines are continually thought up to be put onto the vaccine schedule. Since there is not sufficient benefit to justify the costs or risks of these products, creative marketing, like the moral imperative for herd immunity, needs to be employed to sell the vaccines to a resistant public.
As this article was already quite long, I did not delve into many of the other vaccines which likewise demonstrated the same challenges with attaining herd immunity illustrated by the vaccines discussed here. Although the CDC’s recent decision to add the COVID-19 vaccine to the childhood immunization schedule was egregious and one of the most visible examples of the severe corruption within the agency, I am also quite hopeful this decision will at long last bring these issues into public view.
One promising sign the vaccine zealots overplayed their hand is Tuesday’s ruling by a New York supreme court justice against New York’s vaccine mandates which ordered terminated employees to be reinstated with back pay. Keep in mind that typically judges side with public health officials, especially in liberal states like New York.




0 Comments